Researchers in 2020 performed a meta-analysis to combine the results of studies examining the use of supplements and found an overall improvement in live birth and pregnancy rates, particularly in those using melatonin and CoQ10, but low quality data means more studies must be done.
Women often take antioxidant supplements to improve egg quality, but it’s unclear if this truly has a benefit on pregnancy or live birth rates. I have a more general post on this topic on improving egg quality with supplements, so check it out if you want more background than what’s provided here. Additionally, for more background on egg quality, check out my Complete guide to egg quality.
Showell et al. (2020), in their systematic review and meta-analysis, pool the results of 63 randomized controlled trials (RCTs) examining the impact of antioxidant supplements on pregnancy outcomes, and adverse events. This is an update to their previous 2017 meta-analysis.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Table of Contents
Live birth outcomes
Natural conception and those undergoing fertility treatment (combined)
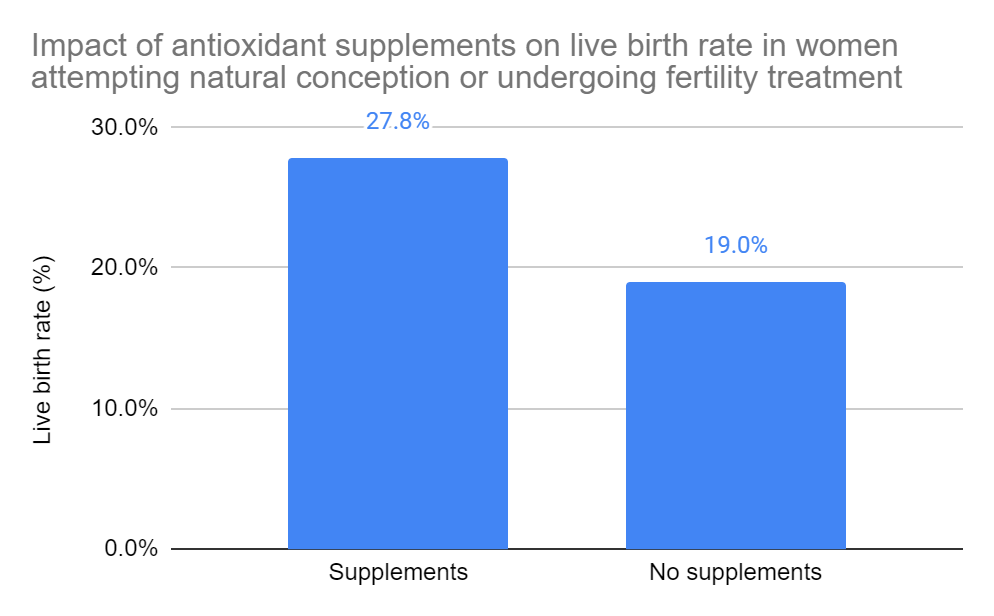
This section looks at how live birth rates changed in women attempting natural conception or undergoing fertility treatment (IUI, IVF, ICSI). All the data is combined until the subgroup analyses (sections below), where IVF and ICSI are examined separately.
Overall impact. Based on 13 RCTs and 1,227 participants, there was a statistically significant increase in live birth rates in women who used antioxidants compared to those who didn’t, or used a placebo (27.8% vs 19.0%, odds ratio [95%] CI: 1.81 [1.36-2.43]). The quality of evidence was very low. This means that the true effect is probably markedly different from what’s been estimated here.
They separated the studies and did a subgroup analysis (below) to see how (1) individual supplements performed, (2) what effect supplements had on women with a particular diagnosis and (3) what effect they had on people only doing IVF or ICSI.
Type of supplement
Note that this is a subgroup analysis from the overall live birth data shown above. All the data here are for women attempting natural conception or undergoing fertility treatment (IUI, IVF, ICSI) – it’s combined. As shown above the quality of evidence is very low.
* indicates a statistically significant difference
*N-acetyl-cysteine. Based on 1 RCT and 60 participants, there was a statistically significant increase in live birth rates in women who used N-acetyl-cysteine compared to those who didn’t, or used a placebo (66.7% vs 40.0%, odds ratio [95%] CI: 3.00 [1.05-8.60]).
L-arginine. Based on 1 RCT and 37 participants, there was no difference in live birth rates in women who used L-arginine compared to those who didn’t, or used a placebo.
CoQ10. Based on 2 RCTs and 225 participants, there was no difference in live birth rates in women who used CoQ10 compared to those who didn’t, or used a placebo.
Vitamin D. Based on 1 RCT and 52 participants, there was no difference in live birth rates in women who used Vitamin D compared to those who didn’t, or used a placebo.
Vitamin B. Based on 2 RCTs and 102 participants, there was no difference in live birth rates in women who used Vitamin B compared to those who didn’t, or used a placebo.
Vitamin E. Based on 1 RCT and 103 participants, there was no difference in live birth rates in women who used Vitamin E compared to those who didn’t, or used a placebo.
Melatonin. Based on 3 RCTs and 270 participants, there was no difference in live birth rates in women who used melatonin compared to those who didn’t, or used a placebo.
*Combined antioxidants. Based on 3 RCTs and 378 participants, there was a statistically significant increase in live birth rates in women who used combined antioxidants compared to those who didn’t, or used a placebo (31.6% vs 16.5%, odds ratio [95%] CI: 2.59 [1.52-4.40]). The combined antioxidants included multiple micronutrients (MMN), vitacap or seidivid. The RCTs for MMN and vitacap showed increases, while seidivid didn’t. There was significant heterogeneity with this analysis (I2=78%).
Diagnosis
Note that this is a subgroup analysis from the overall live birth data shown above. All the data here are for women attempting natural conception or undergoing fertility treatment (IUI, IVF, ICSI) – it’s combined. As shown above the quality of evidence is very low.
* indicates a statistically significant difference
*PCOS. Based on 4 RCTs and 362 participants, there was a statistically significant increase in live birth rates in women with PCOS who used antioxidants compared to those who didn’t, or used a placebo (35.9% vs 17.7%, odds ratio [95%] CI: 3.34 [1.90-5.86]).
Tubal subfertility. Based on 1 RCT and 37 participants, there was no difference in live birth rates in women with tubal subfertility who used antioxidants compared to those who didn’t, or used a placebo.
Unexplained subfertility. Based on 2 RCTs and 133 participants, there was no difference in live birth rates in women with unexplained subfertility who used antioxidants compared to those who didn’t, or used a placebo.
Poor ovarian reserve. Based on 2 RCTs and 266 participants, there was no difference in live birth rates in women with poor ovarian reserve who used antioxidants compared to those who didn’t, or used a placebo.
IVF and ICSI
Note that this is a subgroup analysis from the overall live birth data shown above, and the quality of evidence is very low.
IVF and ICSI. Based on 10 RCTs and 806 participants, there was no difference in live birth rates in women who used antioxidants compared to those who didn’t, or used a placebo (26.3% vs 22.1%, odds ratio [95%] CI: 1.36 [0.96-1.93]).
Clinical pregnancy outcomes
Natural conception and those undergoing fertility treatment (combined)
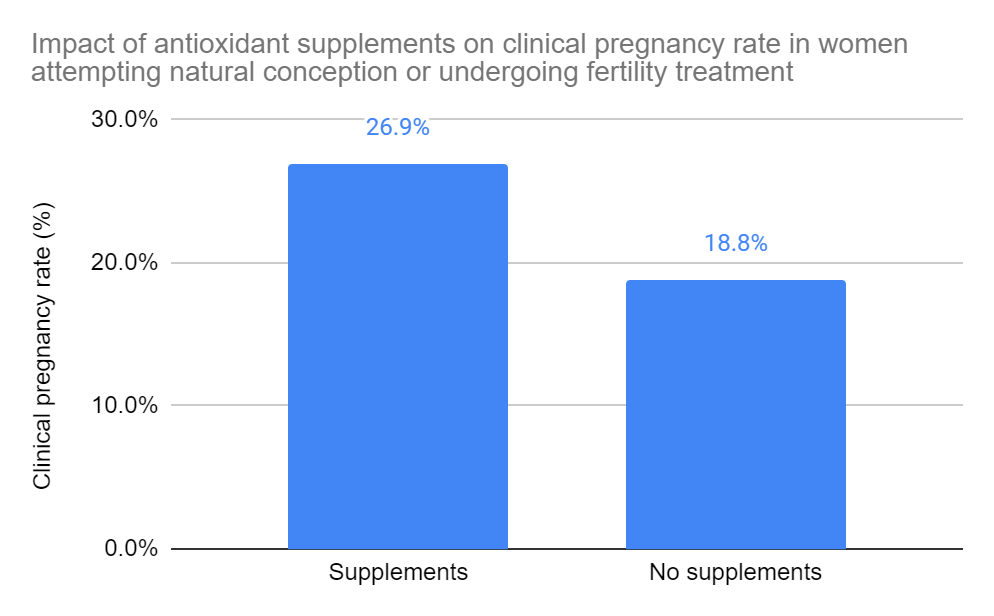
This section looks at how clinical pregnancy rates changed in women attempting natural conception or undergoing fertility treatment (IUI, IVF, ICSI). All the data is combined until the subgroup analyses (sections below), where IVF and ICSI are examined separately.
Overall impact. Based on 35 RCTs and 5,165 participants, there was a statistically significant increase in clinical pregnancy rates in women who used antioxidants compared to those who didn’t, or used a placebo (26.9% vs 18.8%, odds ratio [95%] CI: 1.65 [1.43-1.89]). The quality of evidence was low. This means that the true effect might be markedly different from what’s been estimated here. There was also significant heterogeneity (I2=63%).
They separated the studies and did a subgroup analysis (below) to see how (1) individual supplements performed, (2) what effect supplements had on women with a particular diagnosis and (3) what effect they had on people only doing IVF or ICSI.
Type of supplement
Note that this is a subgroup analysis from the overall clinical pregnancy data shown above. All the data here are for women attempting natural conception or undergoing fertility treatment (IUI, IVF, ICSI) – it’s combined. As shown above the quality of evidence is low.
* indicates a statistically significant difference
*N-acetyl-cysteine. Based on 8 RCTs and 1,590 participants, there was a statistically significant increase in clinical pregnancy rates in women who used N-acetyl-cysteine compared to those who didn’t, or used a placebo (19.8% vs 15.5%, odds ratio [95%] CI: 1.36 [1.05-1.77]). There was significant heterogeneity (I2=71%).
*Melatonin. Based on 7 RCTs and 678 participants, there was a statistically significant increase in clinical pregnancy rates in women who used melatonin compared to those who didn’t, or used a placebo (26.1% vs 19.1%, odds ratio [95%] CI: 1.66 [1.12-2.47]).
Vitamin E. Based on 1 RCT and 103 participants, there was no difference in clinical pregnancy rates in women who used vitamin E compared to those who didn’t, or used a placebo.
Vitamin C. Based on 2 RCTs and 899 participants, there was no difference in clinical pregnancy rates in women who used vitamin C compared to those who didn’t, or used a placebo.
L-arginine. Based on 2 RCTs and 71 participants, there was no difference in clinical pregnancy rates in women who used L-arginine compared to those who didn’t, or used a placebo. There was significant heterogeneity (I2=67%).
Myo-inositol plus folic acid. Based on 1 RCT and 94 participants, there was no difference in clinical pregnancy rates in women who used myo-inositol plus folic acid compared to those who didn’t, or used a placebo.
*CoQ10. Based on 4 RCTs and 397 participants, there was a statistically significant increase in clinical pregnancy rates in women who used CoQ10 compared to those who didn’t, or used a placebo (28.4% vs 14%, odds ratio [95%] CI: 2.49 [1.50-4.13]).
*L-carnitine. Based on 2 RCTs and 450 participants, there was a statistically significant increase in clinical pregnancy rates in women who used L-carnitine compared to those who didn’t, or used a placebo (36.0% vs 4.4%, odds ratio [95%] CI: 11.14 [5.70-21.81]). Note that both these RCTs involved the use of clomiphene with or without metformin. There was significant heterogeneity (I2=85%).
Vitamin D. Based on 2 RCTs and 92 participants, there was no difference in clinical pregnancy rates in women who used vitamin D compared to those who didn’t, or used a placebo.
Vitamin B. Based on 2 RCTs and 102 participants, there was no difference in clinical pregnancy rates in women who used vitamin B compared to those who didn’t, or used a placebo.
Diagnosis
Note that this is a subgroup analysis from the overall clinical pregnancy data shown above. All the data here are for women attempting natural conception or undergoing fertility treatment (IUI, IVF, ICSI) – it’s combined. As shown above the quality of evidence is low.
* indicates a statistically significant difference
*PCOS. Based on 16 RCTs and 1,908 participants, there was a statistically significant increase in clinical pregnancy rates in women with PCOS who used antioxidants compared to those who didn’t, or used a placebo (30.1% vs 11.0%, odds ratio [95%] CI: 4.24 [3.23-5.56]). There was significant heterogeneity (I2=51%).
Unexplained subfertility. Based on 4 RCTs and 997 participants, there was no difference in clinical pregnancy rates in women with unexplained subfertility who used antioxidants compared to those who didn’t, or used a placebo.
Tubal subfertility. Based on 2 RCTs and 71 participants, there was no difference in clinical pregnancy rates in women with tubal subfertility who used antioxidants compared to those who didn’t, or used a placebo. There was significant heterogeneity (I2=67%).
Poor responders. Based on 1 RCT and 65 participants, there was no difference in clinical pregnancy rates in women with poor ovarian response who used antioxidants compared to those who didn’t, or used a placebo.
Poor ovarian reserve. Based on 2 RCTs and 266 participants, there was no difference in clinical pregnancy rates in women with poor ovarian reserve who used antioxidants compared to those who didn’t, or used a placebo.
Endometriosis. Based on 1 RCT and 280 participants, there was no difference in clinical pregnancy rates in women with endometriosis who used antioxidants compared to those who didn’t, or used a placebo.
IVF and ICSI
Note that this is a subgroup analysis from the overall clinical pregnancy data shown above, and the quality of evidence is low.
IVF and ICSI. Based on 19 RCTs and 2,341 participants, there was no difference in clinical pregnancy rates in women who used antioxidants compared to those who didn’t, or used a placebo (29.2% vs 28.5%, odds ratio [95%] CI: 1.15 [0.95-1.40]).
Adverse events
In addition to examining the impact of supplements on live birth and pregnancy rates, the authors combined studies that looked at adverse events. The quality of evidence ranges from moderate to very low. Check the glossary term for quality of evidence to see what these mean.
* indicates a statistically significant difference
Miscarriage. Based on 24 RCTs and 3,229 participants, there was no difference in miscarriage rates in women who used antioxidants compared to those who didn’t, or used a placebo. The quality of evidence was low.
Multiple pregnancy. Based on 9 RCTs and 1,886 participants, there was no difference in multiple pregnancy rates in women who used antioxidants compared to those who didn’t, or used a placebo. The quality of evidence was low.
Gastrointestinal disturbances. Based on 3 RCTs and 343 participants, there was no difference in gastrointestinal disturbances in women who used antioxidants compared to those who didn’t, or used a placebo. The quality of evidence was low.
Ectopic pregnancy. Based on 4 RCTs and 404 participants, there was no difference in ectopic pregnancy rates in women who used antioxidants compared to those who didn’t, or used a placebo. The quality of evidence was low.
Low birth weight. Based on 1 RCT and 160 participants, there was no difference in low birth weights in babies born from women who used antioxidants compared to those who didn’t, or used a placebo. The quality of evidence was very low.
Preterm birth. Based on 2 RCTs and 220 participants, there was no difference in the rate of preterm birth from women who used antioxidants compared to those who didn’t, or used a placebo. The quality of evidence was moderate.
Placenta previa. Based on 1 RCT and 160 participants, there was no difference in the rate of placenta previa in women who used antioxidants compared to those who didn’t, or used a placebo. The quality of evidence was very low.
Preeclampsia. Based on 1 RCT and 160 participants, there was no difference in the rate of preeclampsia in women who used antioxidants compared to those who didn’t, or used a placebo. The quality of evidence was very low.
Conclusions
In women who were trying to conceive naturally or were undergoing fertility treatment:
- Antioxidants showed an overall improvement in live birth and pregnancy rates
- Antioxidants improved live birth and pregnancy rates in women with PCOS.
- N-acetyl-cysteine improved live birth and pregnancy rates.
- Melatonin, CoQ10 and L-carnitine improved pregnancy rates.
In women who were undergoing IVF or ICSI:
- Antioxidant use showed no improvement in live birth or pregnancy rates.
Melatonin and CoQ10 may be effective in improving pregnancy outcomes, while N-acetylcysteine and L-carnitine showed significant heterogeneity (variability in the studies), so it’s less clear if these are effective.
In terms of adverse events, such as miscarriage, ectopic pregnancy and preterm birth, there were no differences in women who took supplements.
In general, the quality of evidence ranged from low to very low. This means that the true impact of supplements “might be” or are “probably” very different from what was found here. We simply do not know the impact of these supplements on pregnancy and live birth rates because the quality of the data is so low.
For the clinical pregnancy studies they found that there was a high risk of publication bias, which could have skewed the results due to the abundance of small studies with positive outcomes. The authors also noted that other reviews on this topic have found high risk of publication bias.
More high quality studies are needed, with a larger sample size, to draw conclusions.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to egg quality
Complete guide to egg quality
 RCT compares fertility outcomes with myo-inositol, probiotic, micronutrient supplements
RCT compares fertility outcomes with myo-inositol, probiotic, micronutrient supplements
 Mediterranean diet and IVF – a clinical trial
Mediterranean diet and IVF – a clinical trial
 Oocyte quality and IVF outcomes linked to maternal lifestyle and diet
Oocyte quality and IVF outcomes linked to maternal lifestyle and diet
 Sleep quality and its impact on IVF outcomes
Sleep quality and its impact on IVF outcomes
 The role of popular diets on fertility and IVF outcomes
The role of popular diets on fertility and IVF outcomes
 CoQ10 and other supplements improve IVF outcomes in women with ovarian aging
CoQ10 and other supplements improve IVF outcomes in women with ovarian aging
 Meta-analysis combines 38 studies on treatments for diminished ovarian reserve
Meta-analysis combines 38 studies on treatments for diminished ovarian reserve