In a 2024 study, researchers developed a model to help predict the number of mature eggs needed to obtain at least one euploid, based on age.
With increasing age, there’s an increased risk of chromosomal errors (aneuploidy) in eggs, and this reduces the chance of getting a euploid by PGT-A. For more information on PGT-A, check out my Complete guide to PGT-A.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This is a retrospective study that took place at a single IVF center in Spain between 2017 and 2022.
- Only trophectoderm biopsies for day 5 and 6 blastocysts were included, using NGS.
- Embryos were graded from A to D, and only blastocysts with qualities A to C were included. D quality is a very low quality ICM or trophectoderm and isn’t normally included as part of standard embryo grading, however refusing to biopsy very low quality embryos is common as this could damage them and potentially kill them.
In terms of sample size, there were 2660 PGT-A cycles, with 92.6% involving women with their own eggs and 7.4% using egg donors.
As age increases, the chance of no euploid or biopsied blastocyst increases
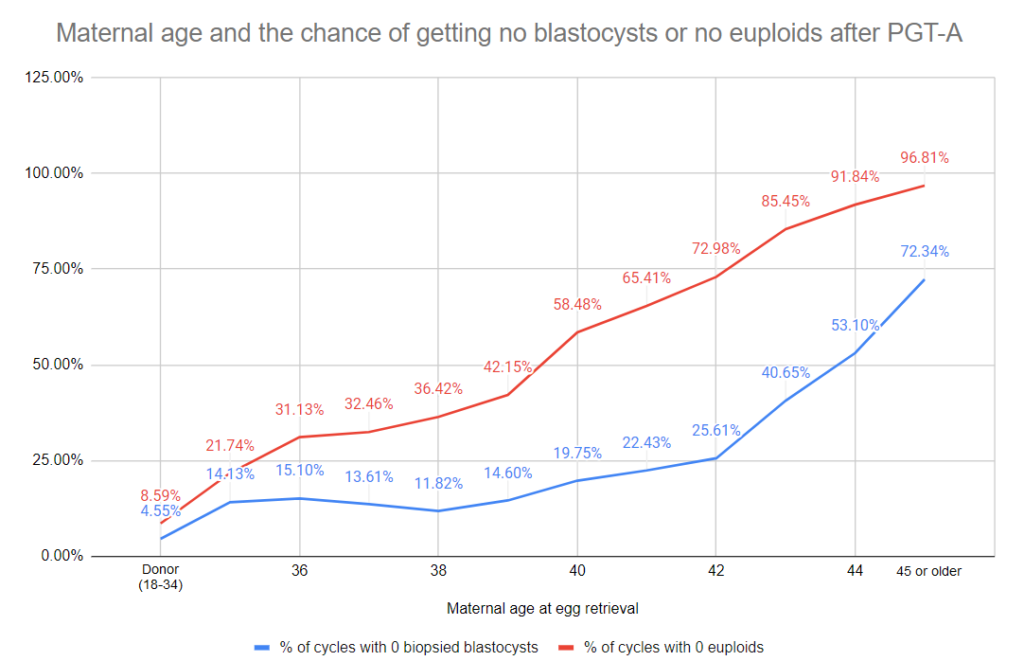
First, the researchers looked at the chance of not getting a euploid, or a blastocyst that was eligible for biopsy (very low quality blastocysts weren’t able to be biopsied). This study involved patients that were 35-45 or older (who used their own eggs) and patients who used donor eggs from donors aged 34 or younger.
As maternal age increased, so did the chance of not getting a euploid or a biopsied blastocyst:
- For the chance of not getting a euploid, this increased from 21.74% at age 35 to 96.81% at age 45 or older. For those using donor eggs, the chance of not getting a euploid was 8.59%.
- For the chance of not getting a biopsied blastocyst, this increased from 14.13% at age 35 to 72.34% at age 45 or older. For those using donor eggs, the chance of not getting a biopsied blastocyst was 4.55%.
As age increases, the number of euploids obtained decreases
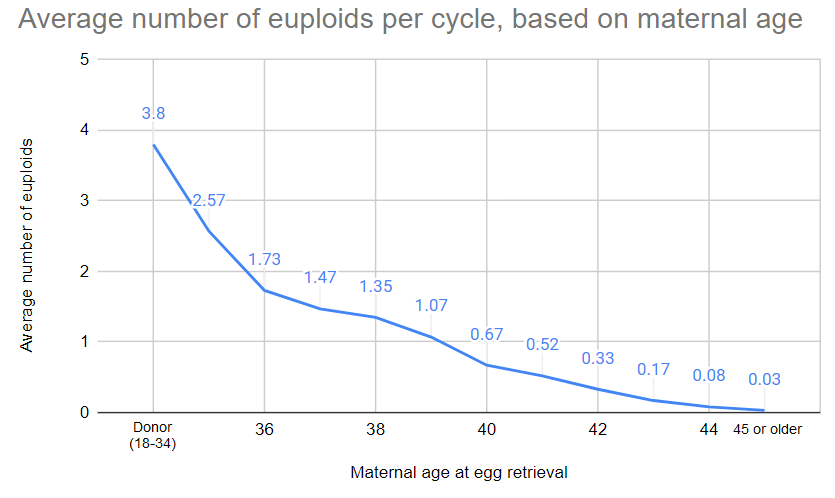
The researchers also reported on the average number of euploids that each patient got from their PGT-A cycle, based on age:
- As age increased, the number of euploids obtained dropped from 2.57 at age 35 to 0.03 at age 45 or older. For those using donor eggs, each cycle produced about 3.8 euploids.
- The patients that used their own eggs had on average 7.9 mature eggs retrieved per cycle, while those using donor eggs had on average 16.4 mature eggs.
As age increases, more mature eggs are needed to obtain at least one euploid
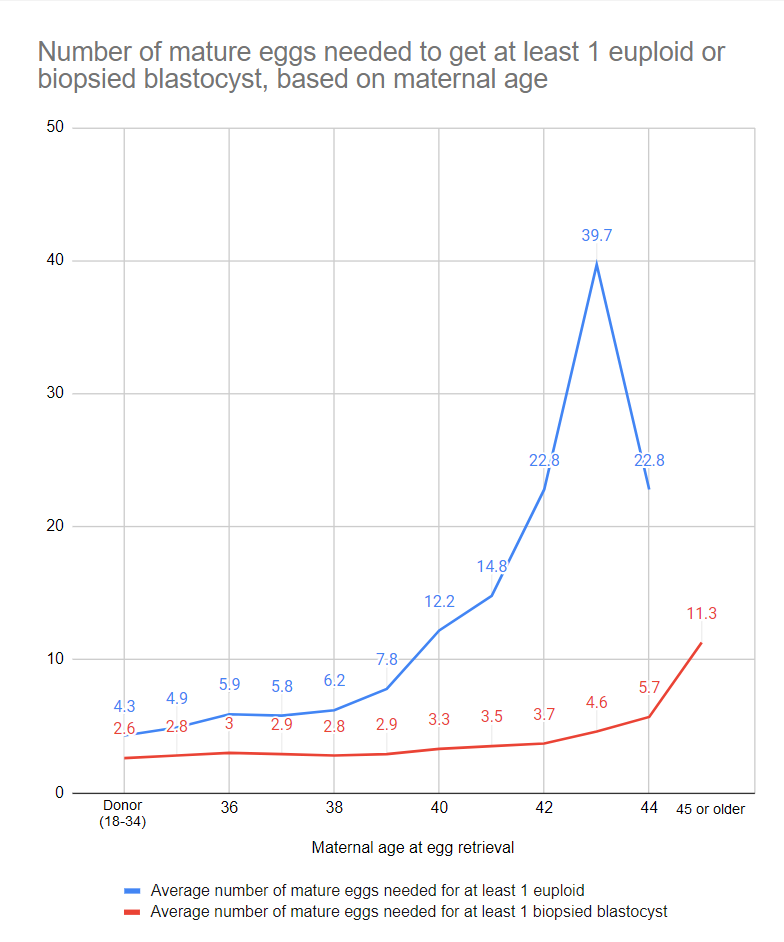
The researchers then calculated the average number of mature eggs needed in order to obtain 1 euploid or 1 biopsied blastocyst.
- For the average number of mature eggs needed for 1 euploid, this increased from 4.9 mature eggs at age 35 to 22.8 mature eggs at age 42 (4.3 for those using donor eggs). Note that the 95% CI (confidence interval) for the number of mature eggs for ages 43 and 44 was very high, so this data is less certain as there is a lot more variability.
- For the average number of mature eggs needed for 1 biopsied blastocyst, this increased from 2.8 at age 35 to 11.3 at age 45 or older (2.6 for those using donor eggs).
Building a model to predict the number of mature eggs needed for at least one euploid, based on age
The last graph shows the average number of mature eggs needed to get a single euploid. Some women may need less while others need more! While this is very useful information, it would be more beneficial to translate these results into a model that predicts the chance of getting a euploid based on the number of mature eggs and age.
So that’s what they did!
Unfortunately, I can’t share an image of the model (a graph) due to copyright restrictions, but I’ll share some of the data from the graph, which I approximated visually:
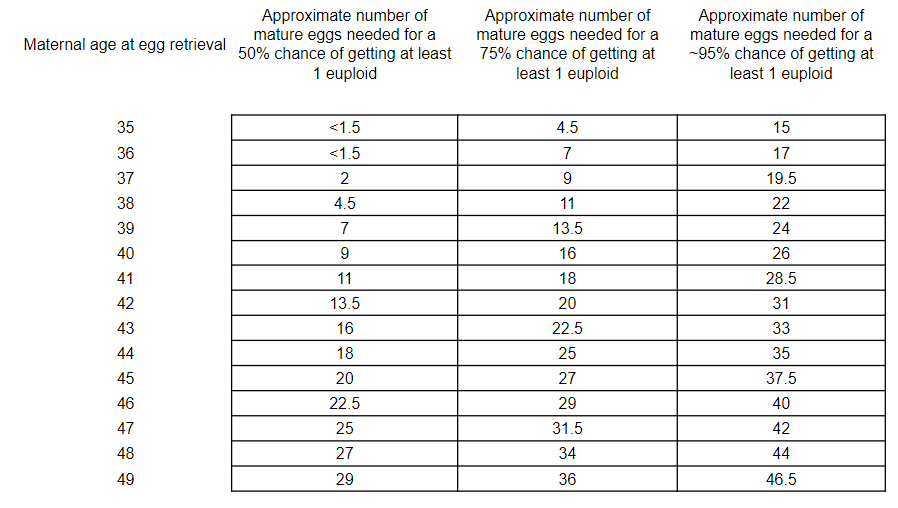
This model takes into account all the patients — from patients who obtained several euploids with few eggs to those who got none despite many eggs. As the chance of getting at least one euploid gets closer to 100% in the model, the number of eggs gets exponentially higher. This is because the model needs to be very conservative to include patients who needed a lot of eggs to get a euploid, while accounting for those who didn’t get any euploids. In other words, the 95% estimates are very conservative, while the 75% estimates are less so.
But how accurate is this model? Is it even worth considering?
They validated their model and found that it had a 72.0% accuracy in predicting patients with at least one euploid. This isn’t very high, and the authors indicate that the model should be optimized and tested in a prospective study in order to be a “trustable clinical tool.”
They performed a multivariate analysis to see which factors contribute to the chance of obtaining at least one euploid. From their list of confounding factors (which they didn’t list), they report that only the age of the egg was significant. This means that of all the possible factors that could influence the chance of getting a euploid, only the age of the egg mattered. This seems a bit of a stretch to me, as things like embryo quality should also contribute, but without more details it’s hard to discuss this further.
Conclusions
This study found that as female age increases:
- The chance of getting a euploid decreases.
- The average number of euploids per cycle decreases.
- The chance of getting a blastocyst that’s eligible for biopsy decreases.
- The average number of mature eggs needed for at least 1 euploid increases — ie. More mature eggs are needed to get at least 1 euploid, as age increases.
Using their data, they built a model to predict the number of mature eggs needed for at least one euploid.
After validation, their model had 72.0% accuracy, which should be optimized before being used as a “trustable clinical tool,” the authors write.
A similar tool was built by another group (referenced below), which included the semen source and other difference, that was externally validated in a separate study. The authors note that their model is based off of much more data, using exclusively NGS-derived PGT-A data, although it must be optimized and validated using another study and in multiple centers before routine use.
Related studies
To learn more about this topic, you can check out a number of studies referenced in this study below (2 links):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Study examines potential of PGT-A on poor quality embryos
Study examines potential of PGT-A on poor quality embryos
 PGT-A meta-analysis finds live birth rates only improve with older patients
PGT-A meta-analysis finds live birth rates only improve with older patients
 Euploid embryos show reduced implantation potential with advancing maternal age
Euploid embryos show reduced implantation potential with advancing maternal age
 Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
 Examining live birth rates in IVF cycles with 5 or less follicles
Examining live birth rates in IVF cycles with 5 or less follicles
 Study compares PGT-A outcomes for patients with different diagnoses
Study compares PGT-A outcomes for patients with different diagnoses
 ASRM’s 2024 committee opinion on the use of PGT-A
ASRM’s 2024 committee opinion on the use of PGT-A
 Study evaluates PGT-A outcomes for good prognosis patients, based on age
Study evaluates PGT-A outcomes for good prognosis patients, based on age