Researchers in a 2022 study performed a meta-analysis to combine the results of PGT-A studies and found no overall improvement in live birth rates across all ages, but an improvement in older women.
PGT-A is often used to select the best embryo for transfer, however it isn’t clear if this technique is better than conventional embryo grading. To learn more, check out my complete guide to PGT-A.
Cheng et al. (2022), in their systematic review and meta-analysis, compared pregnancy outcomes between patients performing PGT-A and those who didn’t. This meta-analysis combined the results of 9 randomized controlled trials (RCTs) that took place between 2013 and 2021.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
No difference in live birth rate with PGT-A (all ages)
Based on 7 RCTs and 3,050 participants across all ages, there was no difference in live birth rates in women who performed PGT-A compared to those who didn’t (57.1% vs 56.2%, risk ratio [95% CI]: 1.13[0.96-1.34]). The quality of evidence was moderate.

They also did a number of sensitivity analyses where they re-analyzed the data to see if they got different results.
To do this they used a different statistical model, or only included trials without a low risk of bias, or excluded the largest trial, or excluded each trial individually.
In all cases, there was no statistical difference in the live birth rate in those who used PGT-A compared to those who didn’t across all ages.
PGT-A improves live birth rate in older women, not younger
This study compared women of advanced maternal age in a subgroup analysis. In general, these were women over the age of 35, however there was overlap between studies as some didn’t differentiate between ages in their analysis or they had a different definition. For example, one study had women 20-37 and was grouped in this meta-analysis as nonadvanced maternal age.
Women with advanced maternal age. Based on 3 studies with 868 participants, there was a statistically significant increase in live birth rates in those who performed PGT-A compared to those who didn’t (36.5% vs 28.3%, risk ratio [95% CI]: 1.34 [1.02-1.77]). The quality of evidence was moderate.
Nonadvanced maternal age. Based on 3 RCTs and 1,746 participants, there was a statistically significant decrease in live birth rates in those who performed PGT-A compared to those who didn’t (69.6% vs 73.4%, risk ratio [95% CI]: 0.94 [0.89-0.99]). The quality of evidence was high. This decrease is small and is probably not clinically significant.
Live birth rates were higher with older PGT-A technology
The researchers grouped the studies based on the type of PGT-A technology used. Next-generation sequencing (NGS) is the standard and has been in use since the mid-late 2010s. Before this, qPCR, aCGH and SNP technology were common. NGS has a higher resolution than these older technologies and can differentiate between mosaics more accurately (low/high level).
NGS technology. Based on 3 RCTs and 2,087 participants, there was a statistically significant decrease in live birth rates in those who performed PGT-A using NGS technology compared to those who didn’t do PGT-A (63.7% vs 67.2%, risk ratio [95% CI]: 0.94 [0.90-1.00]).
Older technology. Based on 4 RCTs and 963 participants, there was a statistically significant increase in live birth rates in those who performed PGT-A using older technology compared to those who didn’t do PGT-A (42.7% vs 32.3%, risk ratio [95% CI]: 1.38 [1.10-1.74]).
The authors didn’t discuss it, but this suggests that newer NGS technology has worsened outcomes compared to older technology, however the small difference is probably not clinically meaningful.
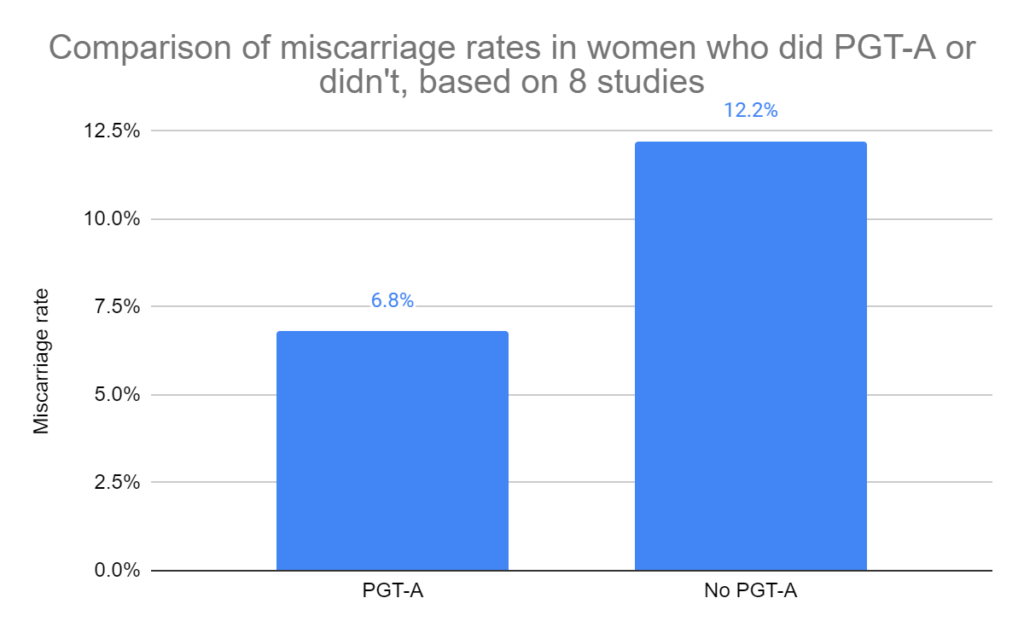
PGT-A reduces miscarriage rates
Based on 8 RCTs and 3,129 participants, there was a statistically significant decrease in miscarriage rates in those who performed PGT-A compared to those who didn’t (6.8% vs 12.2%, risk ratio [95% CI]: 0.53 [0.35-0.81]). The quality of evidence was moderate.
No difference in clinical pregnancy or ongoing pregnancy rates in those doing PGT-A
Based on 7 RCTs and 2,460 participants, there was no difference in clinical pregnancy rates in women who performed PGT-A compared to those who didn’t (67.7% vs 73.7%, risk ratio [95% CI]: 0.96 [0.86-1.07]). The quality of evidence was moderate.
Based on 6 RCTs and 2,563 participants, there was no difference in ongoing pregnancy rates in women who performed PGT-A compared to those who didn’t (62.4% vs 61.5%, risk ratio [95% CI]: 1.20 [0.96-1.50]). Ongoing pregnancy was defined as a pregnancy beyond 12 weeks. The quality of evidence was low.
No difference in multiple pregnancy rates with PGT-A
Based on 5 RCTs and 2,123 participants, there was no difference in multiple pregnancy rates in women who performed PGT-A compared to those who didn’t (2.5% vs 3.5%, risk ratio [95% CI]: 0.86 [0.38-1.92]). The quality of evidence was moderate.
No differences in birth weight of babies born from PGT-A
Based on 3 RCTs and 1,177 participants, there was no difference in the birth weight of babies born from women who performed PGT-A compared to those who didn’t (average difference [95% CI]: 45.74 [-44.52 – 136.00]).
Conclusions
This study found no difference in live birth rates in women pursuing PGT-A, but there was a decrease in miscarriage rates. When they grouped participants by age, there was an improvement in live birth rates in older women only.
Even though conventional grading may select an embryo just as well as PGT-A in some cases, a benefit of PGT-A is identifying which embryos are aneuploid. Aneuploid embryos have a very low chance of producing a live birth, so even in younger women PGT-A may be desirable.
There were several limitations in this study.
One was that there was a high amount of variability in the studies (heterogeneity) which was due to the difference ages of women.
There were also differences in how some of the studies were designed. For example, some studies included only one transfer with euploids against a highly graded embryo embryo, while one study compared cumulative rates after transferring up to 3 euploids.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Study examines potential of PGT-A on poor quality embryos
Study examines potential of PGT-A on poor quality embryos
 Euploid embryos show reduced implantation potential with advancing maternal age
Euploid embryos show reduced implantation potential with advancing maternal age
 Study evaluates factors affecting pregnancy outcomes after euploid transfer
Study evaluates factors affecting pregnancy outcomes after euploid transfer
 Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
 Study compares PGT-A outcomes for patients with different diagnoses
Study compares PGT-A outcomes for patients with different diagnoses
 IVF outcomes following aneuploid embryo transfer
IVF outcomes following aneuploid embryo transfer
 Multiple embryo freeze/thaw for PGT-A doesn’t affect pregnancy or neonatal outcomes
Multiple embryo freeze/thaw for PGT-A doesn’t affect pregnancy or neonatal outcomes
 A look at how PGT-A results change with age, using data from over 86,000 biopsies
A look at how PGT-A results change with age, using data from over 86,000 biopsies