
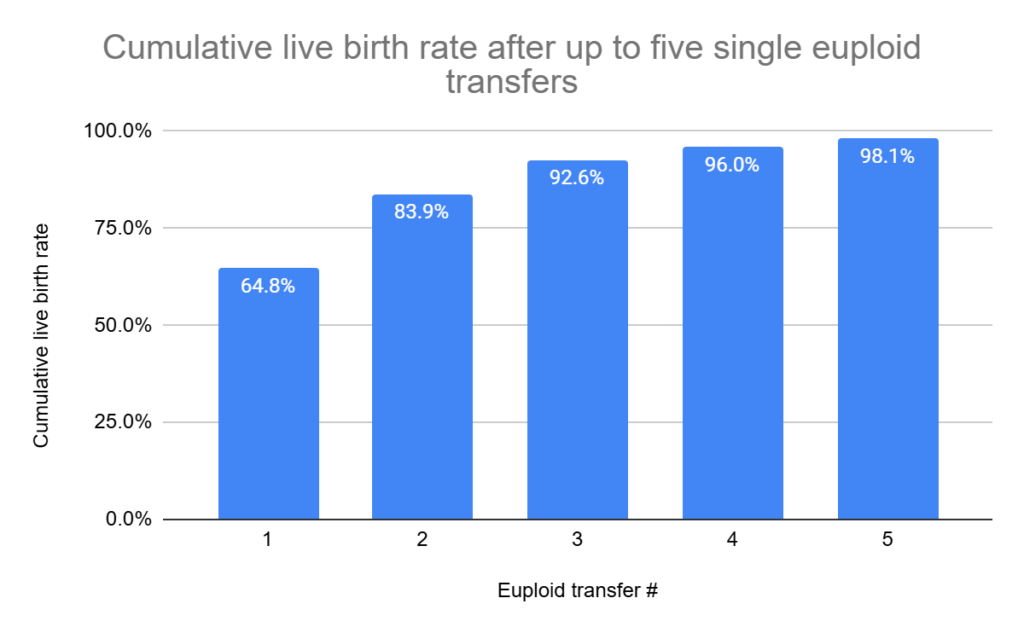
Researchers in a 2024 study found that patients that have 5 consecutive euploid transfers had a cumulative live birth rate of 98.1%, suggesting that most cases of implantation failure are due to the embryo, and that true unexplained RIF occurs in less than 2% of patients.
RIF describes patients that have consistent implantation failure due some underlying factor. There’s no consensus on the number of implantation failures needed for RIF, although most agree with 3 failed fresh or frozen transfers. The choice of 3 failed transfers for RIF is arbitrary, and “true” cases of RIF have consistent failures as a result of some underlying cause that’s unexplained.
Embryo quality can definitely contribute to implantation failure, so to better understand how common true RIF really is, this study follows the outcomes of patients with up to 5 euploid embryo transfers. This study, by Gill et al. (2024), is a continuation of a previous study in 2020 that followed women who had 3 consecutive euploid transfers.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This was a retrospective, international, multi-center study performed at 26 clinics in the US, Spain, Italy and the UAE between 2012 and 2022.
- Patients had RIF and had failed to achieve a pregnancy after transferring a single euploid three times.
- Double euploid transfers were permitted, as long as both embryos failed to implant or did implant (so they could be tracked).
- Patients with obvious causes of implantation failure were excluded, such as those having karyotype abnormalities, uterine anomalies (fibroids, polyps, adenomyosis, a thin endometrium) and non-obstructive azoospermia in the male partner. Additional exclusions involved the use of donor eggs, mosaic embryo transfers, and more. All transfers had to have been done at one of the 26 clinics.
- Most clinics used NGS for testing, but one used qPCR.
- The primary outcomes were clinical pregnancy and live birth rate after the 4th and 5th euploid transfer.
Pregnancy outcomes for the 4th and 5th euploid transfers
There were 123,987 patients who had 64,572 euploid transfers. Of these transfers, there were 105 patients who had 3 failed euploid transfers that went on to have a 4th and 5th euploid transfer.
Of the 105 patients who had a 4th euploid transfer, 54 became pregnant and 42 had a live birth (51.4% clinical pregnancy rate and 40% live birth rate).
There were 45 patients who had a 5th euploid transfer, with 28 pregnancies and 24 live births (62.2% clinical pregnancy rate and 53.3% live birth rate).
The pregnancy and live birth rates were similar between clinics. There were no statistical differences between the outcomes of the 4th or 5th transfers.
In terms of the cumulative live birth rates for euploid transfers 1-5 (note that I needed to visually estimate transfer 4’s result from a graph):
This study is a continuation of a previous study from Pirtea et al. 2020 based on data from one of the clinics (RMA New Jersey), which compared outcomes of the patients who had up to 3 euploid transfers. In the current study, they compared the 1st and 4th euploid transfer, and found there was no difference in live birth rates. They didn’t have a high enough sample size to compare the 5th transfer.
They also did sensitivity analyses to assess the data differently, including an analysis with day 7 blastocysts, women with a high BMI, those using the ERA test, and more. All analyses showed similar results.
Conclusions
The overall cumulative live birth rate after 5 euploid transfers was 98.1%. This means that 98.1% of women who had up to 5 euploid transfers had a live birth, and that RIF (with 5 failed euploid transfers) occured in about 2% of patients.
It’s important to stress that there were no additional treatments and only a euploid embryo was transferred. This suggests that the embryo itself is the cause for the majority of cases of implantation failure and true RIF is relatively rare.
This study found no difference in the live birth rates between the 4th and 5th euploid transfer. There was also no difference between the 1st and 4th transfer.
This last point is interesting because we would expect success rates to drop with successive euploid transfer cycles, as patients with true RIF become enriched with each cycle.
For example, let’s say there’s 1,000 patients: 900 without RIF that have a 50% chance of live birth, and 100 that have true RIF and consistently have implantation failure.
- After the first transfer, 450/900 and 0/100 have a live birth. The overall live birth rate is 450/1000 = 45%. Now there’s 900-450 = 450 non-RIF patients for the second transfer.
- After the second transfer, 225/450 and 0/100 have a live birth. The overall live birth rate is 225/550 = 40.9%.
- After the third transfer, 112/225 and 0/100 have a live birth. The live birth rate is 112/325 = 34.5%.
And so on. As the number of patients without RIF keep having success and dropping out, the true RIF patients continue to enrich the overall group of IVF patients. This lowers the overall live birth rate after each transfer.
But this isn’t what we’re seeing in this study!
Instead, after each transfer attempt, the chances of live birth are the same. This suggests that the true RIF group is very small and that most patients have about a 50% chance of success. Since the patients going into this study had RIF by definition (they had 3 previous failed euploid transfers), this study also suggests that about half* of the RIF cases can be resolved by another euploid transfer (*the live birth rate after the 4th transfer was close to half).
Having 3 failed transfers for RIF is kind of ambiguous and there’s a lack of consistency in how RIF is defined. There’s even debate as to whether or not it’s a real condition! Cimadomo et al. (2021) performed a survey among clinicians and embryologists and found that the most common definition is 3 failed fresh or frozen transfers. The ESHRE good practice recommendations on RIF (2023) challenges this definition, stating that it doesn’t take into account individual patient- or clinic-related variables, and that “the concept of RIF as a syndrome or disease that can be diagnosed and treated is open to challenge.” Part of the challenge I think is that RIF can ultimately be attributed to some diagnosis, although this diagnosis may not be obvious (for example, a faulty gene that no one knows about).
So after this research, is it still worth it to define RIF as 3 failed transfers? Or should it be increased? Should failed euploid transfers be a requirement for RIF?
I think the 3 failed transfers for RIF is still useful as an initial diagnosis, to open the door to more tests that could lead to a better diagnosis. However, treating RIF with IVF add-ons have conflicting data, leading ESHRE to not recommend their use. Maybe it’s because about half of RIF patients would have had success anyway, without further treatment, as suggested by this study?
So why do some patients have success their first try, compared to other patients who take several tries? It seems like there’s some unfavorable uterine condition that prevents implantation, that for some reason is resolved in about 50% of patients who have another transfer attempt. Is this related to the window of implantation, the immune system, or something else?
What happens when patients have 6, 7 or more euploid transfers? Is there a certain number of failed euploid transfers where there is no longer an increase in the cumulative live birth? Will a group of patients always have the same chance with each round of euploid transfer? What’s the true incidence of true RIF?
To be clear, this study isn’t suggesting that patients have 5 euploid transfers. It’s trying to determine how common true RIF is. In other words, in a population of patients without obvious causes of implantation failure, is there still a group that consistently has implantation failure?
This study could have found an answer, if there was no improvement beyond a certain number of transfers. So if the cumulative live birth rates peaked after 3 euploid transfers at 92.6%, and no additional euploid transfers increased the cumulative rate, this would tell us that there’s a group that makes up about 7% of the population that doesn’t have any obvious causes of implantation failure AND doesn’t respond to euploid transfers. This would have been valuable information because it would have identified a group of true RIF patients that could help advance diagnosis and treatment efforts. But this wasn’t the case. Instead, we’re seeing that each transfer gives about the same chance of success as the previous transfers, and there doesn’t seem to be a true RIF group, or it’s rare and can’t currently be detected. Having more transfers would help to find this group, but it’s difficult given how uncommon it is for a patient to have 5 or more consecutive euploid transfers.
So many questions! Regardless, I think it’s reassuring that most patients can have success without additional treatments. Of course, getting more euploid embryos to transfer is a separate challenge!
There were some limitations of this study:
- It was retrospective.
- It’s possible that patients who choose to continue trying another euploid transfer are in some way different from those patients that choose to stop. The patients that continue may have a higher ovarian reserve, for example.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?
 Whole exome sequencing used to identify 6 genes involved in recurrent euploid miscarriage
Whole exome sequencing used to identify 6 genes involved in recurrent euploid miscarriage
 Meta-analysis of commonly used IVF immunotherapies shows no benefit
Meta-analysis of commonly used IVF immunotherapies shows no benefit
 Aneuploid-only first PGT-A cycle has no impact on future PGT-A outcomes
Aneuploid-only first PGT-A cycle has no impact on future PGT-A outcomes
 RCT finds no change in birth rates for standard or ERA-timed euploid transfer
RCT finds no change in birth rates for standard or ERA-timed euploid transfer
 Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
 Study compares PGT-A outcomes for patients with different diagnoses
Study compares PGT-A outcomes for patients with different diagnoses
 Silent insulin resistance is common, linked to lower IVF success rates
Silent insulin resistance is common, linked to lower IVF success rates