A new study compared cumulative live birth rates for patients based on their age, the number of eggs retrieved and diagnosis. They found that age had the strongest impact on live birth rates.
Cumulative live birth rates (CLBR) refer to the overall chance of a live birth after a number of transfers. It often refers to the overall chance after transferring all available embryos.
This post is a summary of a study by Zeng et al. (2024), involving women who had 5 or more frozen transfers using untested embryos. All the embryos weren’t necessarily transferred in this study, but it still gives us a good look at how CLBRs change with age and other criteria.
This study analyzes CLBR after at least five frozen embryo transfers. Since some women didn’t do this many transfers (and had embryos leftover) the researchers used two methods to estimate the “true” CLBR:
- Optimistic Method: Calculates the highest possible CLBR. It assumes women who stop transfers early would have had the same chance of a live birth as those who continued with more transfers.
- Conservative Method: Calculates the lowest possible CLBR. It assumes that if a woman stops treatment, she has no further chance of live birth.
Basically, it gives us an upper limit (the best case scenario — optimistic) and a lower limit (worst case scenario — conservative) for the CLBR — with the true value somewhere in between.
They looked at CLBR based on age, the number of eggs retrieved, and diagnosis.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This is a retrospective study that took place between 2010 and 2023 at a single IVF center in China.
- One to two embryos were transferred, either day 3 or good quality day 5 or 6 embryos. There was no indication that PGT was done, so these were most certainly untested embryos.
- Women could have had more than one egg retrieval cycle: 49.8% had one cycle, 20.6% had two, 8.8% had three, 4.8% had four and 7.3% had five.
- Women could have had more than one FET: 49.8% had one FET, 28.9% had two FETs, 12.6% had three FETs, 5.1% had four FETs and 3.6% had five or more FETs.
- The primary outcome was the CLBR, after all egg retrievals and FET cycles.
In terms of sample size, there were a total of 43,972 women that had 86,496 egg retrieval cycles and 82,022 FET cycles:
- Aged <30: 12,861 women
- 30-34: 17,772
- 35-39: 9192
- 40-42: 2557
- 43-44: 953
- ≥45: 637
Cumulative live birth rates based on age, after 5 or more frozen transfers
In the first part of the study, they looked at cumulative live birth rates (CLBR) based on female age, after 5 or more frozen transfers. Let’s look at both the optimistic (upper limit) and conservative (lower limit) methods, as described earlier. We’ll start with the optimistic method and walk through it so you can understand it.
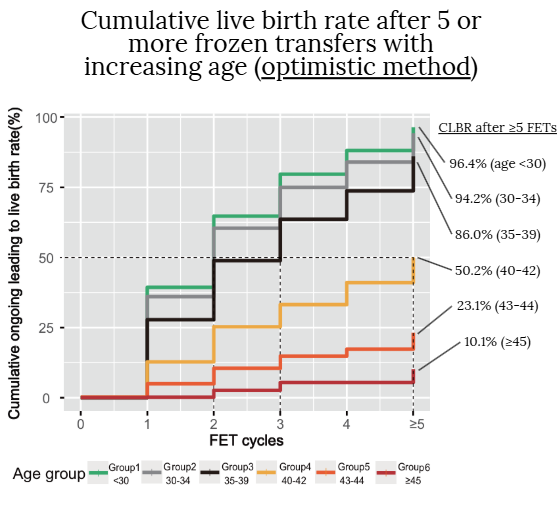
- Focusing on the red line on the bottom (age ≥45) — we see that for FET 1 there’s no increase in the CLBR. The CLBR slightly rises with FET 2, sees another small increase with FET 3, remains unchanged with FET 4, and then slightly increases again with FET ≥5.
- With FET ≥5, it increases to 10.1%. This means that after 5 or more total FETs, there was a 10.1% chance of live birth for women aged ≥45. I drew a line from the top of the red line for FET ≥5. Note: Only 3.6% of women in this study had five or more FETs, so most of the information about live birth rates mainly covers the first four FETs. I highlight this because the researchers grouped everyone with five or more FETs into a single category (FET ≥5). This grouping makes it unclear exactly when the CLBR increases—was it after the fifth, sixth, or seventh FET? With FET 4, we know exactly what the CLBR is. Unfortunately, this study only reports on the exact percentages for FET ≥5, so you’ll have to use your best judgment to figure out what the graph says for FET 4, 3, etc.
- For the other ages with the optimistic method, the CLBR after 5 or more FETs is 96.4% (<30), 94.2% (30-34), 86.0% (35-39), 50.2% (40-42), 23.1% (43-44) and 10.1% (≥45).
Alright! Now that we’re pros and can analyze these graphs, let’s look at the conservative method. Remember, the optimistic method above is the upper limit (best case scenario) for CLBR, and the conservative method below is the lower limit (worst case scenario).
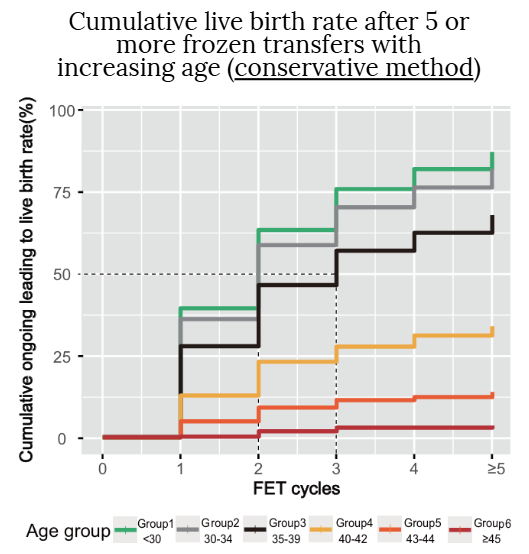
- For the conservative method, the CLBR after 5 or more FETs was 87.1% (<30), 82.0% (30-34), 67.8% (35-39), 33.9% (40-42), 13.8% (43-44) and 3.5% (≥45).
Now we can put it together! I’ll list the lower limit and upper limit below for five or more FETs (FET ≥5). The true CLBR is in between these values:
- Age <30: 87.1% – 96.4%
- 30-34: 82.0% – 94.2%
- 35-39: 67.8% – 86.0%
- 40-42: 33.9% – 50.2%
- 43-44: 13.8% – 23.1%
- ≥45: 3.5% – 10.1%
Based on these results, the authors made the following conclusions:
- Women up to 39 years old see increased chances of having a baby with each additional embryo transfer.
- Women between 40 and 44 years old may not see much improvement in their chances after three transfers.
- Women older than 45 may consider stopping after three transfers, as their chances of success do not significantly increase beyond that point.
- As women get older, the likelihood of transferring embryos with the wrong number of chromosomes (aneuploid embryos) increases, which might explain why there are no further increases in success rates. However, when chromosomally normal (euploid) embryos are transferred, the impact of age on embryo quality is essentially negated. If only euploid embryos were used, we wouldn’t expect to see the CLBR to flatten out.
So this gives us a good picture for what women can expect after having five or more transfers. However, some might want to know what the CLBRs look like for fewer FETs. Let’s say we want to look for the CLBR after 2 FETs, for someone who’s 35-39. To do this, look at the optimistic graph above: for 35-39 (black curve) FET 2 is about 50% — this is the upper limit. Next, look at the conservative graph: it looks like it’s just a bit below 50%, so let’s say about 45% — this is the lower limit. Putting it together, the CLBR for 2 FETs for someone aged 35-39 is between 45% – 50%. In other words, women aged 35-39 who have two FETs have an overall (cumulative) chance of live birth between 45% – 50%.
Cumulative live birth rates based on the number of eggs retrieved, after 5 or more frozen transfers
Besides age, they also looked at CLBR and the number of eggs retrieved. Having more eggs retrieved means more chances at having embryo transfers. There’s also some evidence that suggests getting more eggs means higher overall egg quality.
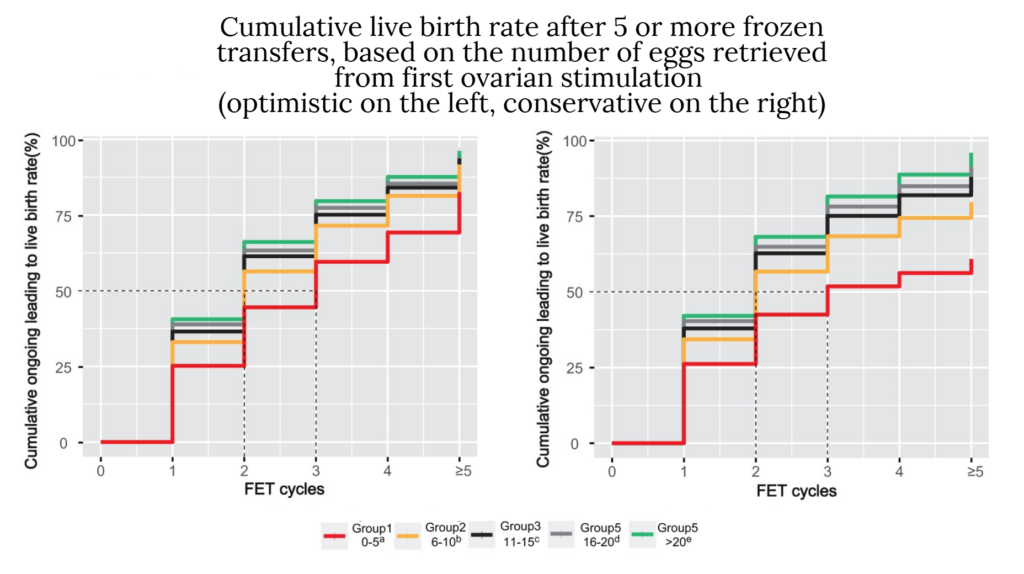
Below are the lower and upper limits for five or more FETs (FET ≥5) based on the number of eggs retrieved from the first retrieval. The true CLBR is in between these values:
- 0-5 eggs retrieved after first ovarian stimulation: 58.6% – 82.5%
- 6-10: 82.0% – 76.7% – 91.7%
- 11-15: 67.8% – 84.8% – 93.6%
- 16-20: 33.9% – 88.0% – 94.1%
- ≥20: 92.5% – 96.2%
So we can see here that women who have a lot of eggs retrieved after their first ovarian stimulation have a higher CLBR.
Cumulative live birth rates based on diagnosis, after 5 or more frozen transfers
They also compared CLBRs based on diagnosis!
- Tubal Factor: Issues such as blocked fallopian tubes, fluid in the tubes (hydrosalpinx), or past tubal surgeries that prevent pregnancy.
- Male Factor Infertility: Includes problems like reduced sperm motility (asthenozoospermia), low sperm count (oligospermia), abnormal sperm shape (teratozoospermia), sexual dysfunction, and retrograde ejaculation.
- Polycystic Ovary Syndrome (PCOS): A condition diagnosed when with irregular or absent ovulation, high levels of male hormones causing symptoms like excessive hair growth, or multiple cysts on the ovaries.
- Diminished Ovarian Reserve (DOR): A reduction in both the quality and quantity of a woman’s eggs, indicated by low levels of AMH, few antral follicles in the ovaries, and high levels of FSH.
- Endometriosis: The presence of tissue similar to the uterine lining outside the uterus, which can cause pain and affect fertility, usually diagnosed through symptoms and confirmed via laparoscopy.
- Uterine Factors: Includes conditions like adhesions (scar tissue inside the uterus), polyps, inflammation, anomalies in the shape or structure of the uterus, fibroids (benign tumors in the uterine wall), or adenomyosis (endometrial tissue growing into the uterine muscle).
- Combined Causes: Infertility that involves two or more of the above issues, making diagnosis and treatment more complex.
- Unexplained Infertility: A situation where all fertility tests are normal, and there’s no identifiable cause for infertility despite regular unprotected sex.
- Other Infertility: Includes factors not covered by other categories, such as advanced age, a history of recurrent miscarriages, or unsuccessful IVF attempts at other medical facilities.
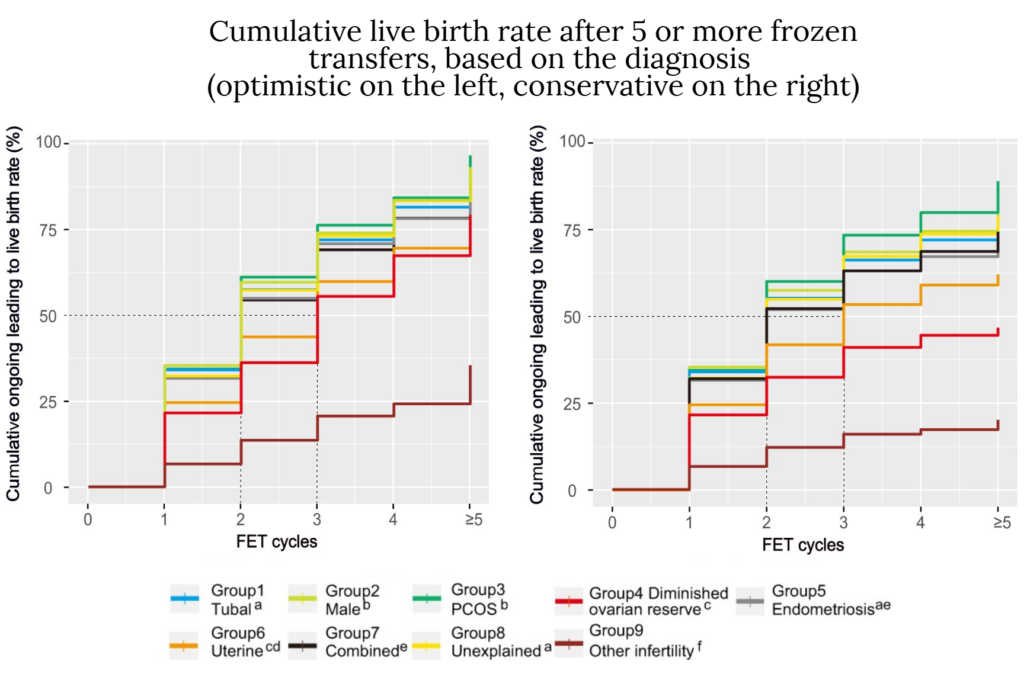
Below are the lower and upper limits for five or more FETs (FET ≥5) based on the diagnosis. The true CLBR is in between these values:
- Tubal Factor: 77.3% – 91.7%
- Male Factor Infertility: 79.4% – 93.1%
- PCOS: 88.9% – 96.6%
- DOR: 46.7% – 79.2%
- Endometriosis: 72.7% – 89.9%
- Uterine Factors: 62.1% – 76.1%
- Combined Causes: 74.4% – 90.0%
- Unexplained Infertility: 78.8% – 92.9%
- Other Infertility: 20.1% – 35.4%
The ranking order (from best CLBR to worst): PCOS, male factor, unexplained infertility, tubal factor, endometriosis, combined factors, uterine factor, DOR, and other infertility.
Conclusion
Female age had the strongest impact on CLBR. Women aged 40-44 saw a small increase in their chances after three transfers, but for women 45 and older, there was no improvement after three transfers. It’s important to remember that untested embryos were transferred, many of which were likely aneuploid with increasing age. If euploids were transferred, we would expect the CLBR to increase, even in older women. The challenge, of course, is getting euploid embryos at that age — studies show that embryos are more likely to be aneuploid with increasing age.
This isn’t the point of this study, or other studies on CLBR, because what we’re trying to see is what the chances are for women who are simply transferring what they get (and not testing their embryos). Other studies have shown that the impact of age is minimized when transferring euploids, so we might expect that the CLBR would keep increasing in a similar way across all ages. By including euploids in this study, it would give us different results and would mask what would naturally occur by transferring untested embryos.
This aligns with other studies on age and CLBR. For instance, one study indicated that the highest CLBR for women aged 40-42 occurred around the eighth transfer, while for women aged 43 and older, it peaked at around the second or third transfer (reviewed in my post Cumulative live birth rates in women aged 40+, after up to 10 transfers). Another study suggested that women aged 43 and 44 reached their highest CLBR around the fifth egg retrieval cycle, and for women aged 45 and 46, it was around the second cycle (reviewed in my post Cumulative live birth rates in women aged 43+, after up to 10 cycles). I’ll link some other studies below.
For the number of eggs retrieved (after the first ovarian stimulation cycle), women who retrieved more eggs generally had a higher CLBR.
For diagnosis, the CLBR was highest for women with PCOS and lowest for women with DOR and other infertility. Women with DOR would have fewer eggs retrieved, and fewer embryos available to transfer, which might explain the lower CLBR.
Related studies
To learn more about this topic, you can check out a number of studies referenced in this study below (5 links):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Sleep quality and its impact on IVF outcomes
Sleep quality and its impact on IVF outcomes
 Cumulative live birth rates in women aged 40+, after up to 10 transfers
Cumulative live birth rates in women aged 40+, after up to 10 transfers
 Egg freezing and thawing
Egg freezing and thawing
 Study finds poor ovarian responders have no further live births after 4 cycles
Study finds poor ovarian responders have no further live births after 4 cycles
 No differences in IVF outcomes when using fresh or frozen donor eggs
No differences in IVF outcomes when using fresh or frozen donor eggs
 Pilot study shows improved IVF outcomes after spindle transfer in women with poor egg quality
Pilot study shows improved IVF outcomes after spindle transfer in women with poor egg quality
 Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
 Early triggering with the “HIER” protocol may be a better approach for older women
Early triggering with the “HIER” protocol may be a better approach for older women