
Researchers in a 2023 study found that women who waited at least 6 months between a clinical pregnancy loss and an FET had improved outcomes compared to women who waited less time.
This study looked at patients who had a clinical pregnancy loss (not a biochemical loss) and then had a frozen embryo transfer (FET) within a year. Patients were grouped based on how long they waited until that FET. They wanted to see if patients who waited longer had a higher live birth rate or not.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This was a retrospective study that took place between 2017 and 2022 at a single IVF center in China.
- After their clinical loss, patients had an FET within a year using an embryo from the same retrieval.
- Exclusions: Patients with recurrent pregnancy loss, recurrent implantation failure (RIF), uterine abnormalities, PGT-A, donor eggs or frozen eggs.
There were a total of 2,433 patients in this study. They were grouped based on the length of time from their loss to their FET:
- <3 months: 338 patients
- 3 to <6 months: 1,347 patients
- 6 to 12 months: 748 patients
In terms of the patient’s baseline characteristics, there were differences in patients 35 or older*, parity, PCOS diagnosis, AMH levels*, fertilization method (IVF/ICSI), FET protocol used, and more. These were statistically adjusted in their analysis.
* The average age was ~32 between the groups, but there were more patients 35 or older in the <3 months group (33.7% vs 28.2% and 26.1%, p= 0.03). The <3 month group also had a lower AMH (3.0 vs 3.8 and 3.8).
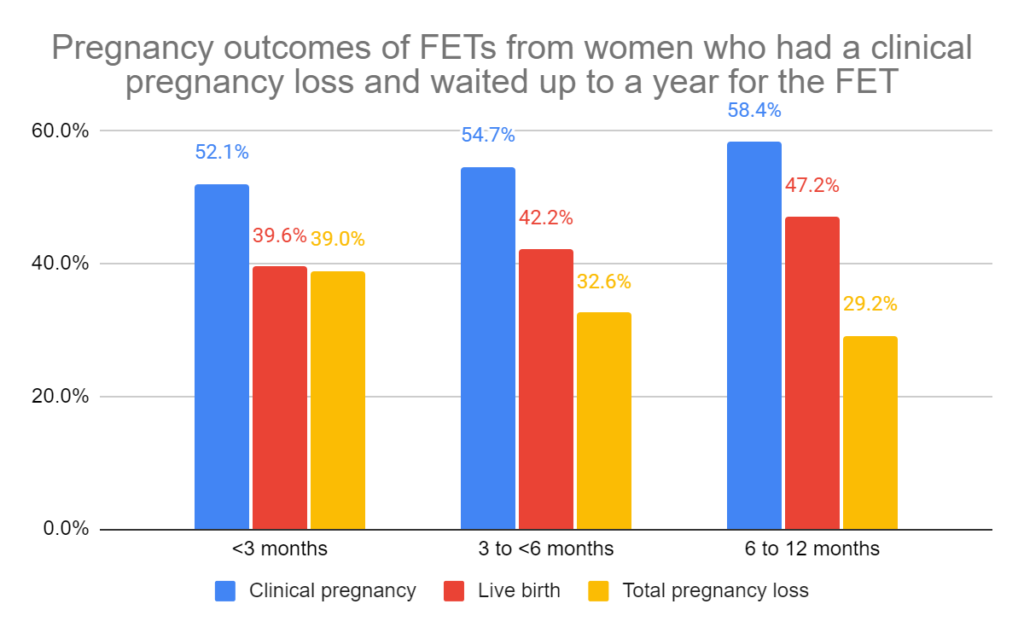
Live births were highest in patients with a 6-12 month interval between clinical pregnancy and a clinical loss
Live birth rates were highest in the 6-12 month group vs the 3 to <6 month and <3 month group (47.2% vs 42.2%, 39.6%, p= 0.03; adjusted odds ratio [95% CI]: 0.64 [0.48-0.85]; 0.74 [0.61-0.90])).
There was also an increase in clinical pregnancies for the 6 to 12 month group, compared to the <3 month and 3 to <6 month group (58.4% vs 54.7%, 52.1%, p= 0.10*; adjusted odds ratio [95% CI]: 0.70 [0.53-0.92]; 0.79 [0.65-95]). *Note that this was only statistically significant after adjustment..
For total pregnancy losses (biochemical + clinical losses), there was a decrease in the 6 to 12 month group compared to the <3 month and 3 to <6 month group (29.2% vs 32.6%, 39.0%, p= 0.04; adjusted odds ratio [95% CI]: 1.87 [1.31-2.67], 1.29 [1.00-1.66].
There were no differences in preterm births or birthweights between the groups.
Conclusions
Women who waited 6 to 12 months after a loss had an improved chance of live birth compared to those who waited <3 months and 3 to <6 months (47.2% vs 39.6% and 42.2%).
There was also an improvement in clinical pregnancy rates, and a decrease in total pregnancy loss (which included both biochemical and clinical losses).
The optimal waiting time after a loss is a topic of debate, with some studies suggesting that waiting at least 6 months may not be necessary. However, much of this data is based on unassisted conception.
It’s not clear why a shorter interval would have a negative effect on pregnancy, but it may be due to inadequate physical and psychological recovery from a previous loss, the authors write. For instance, there could be endometrial damage from a D&C, changes in the uterine microbiome, or post-traumatic stress after a loss.
The authors listed some limitations.
- The <3 month group had more older women, potentially affecting the results, even though they tried to control for it.
- Number of previous transfers might have affected the results, which they didn’t look at (but they did exclude RIF patients).
This research shows that waiting at least 6 months after a loss may improve FET outcomes. However, more evidence is needed to confirm this.
Related studies
Not all research may agree with this study. There were a number of studies referenced in this study that you might want to check out, as shown below (6 links):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Study examines transferring a good and poor quality embryo together
Study examines transferring a good and poor quality embryo together
 Why do embryos in IVF fail to implant or miscarry?
Why do embryos in IVF fail to implant or miscarry?
 Endometrial thickness and pregnancy outcomes after 96,000 embryo transfers
Endometrial thickness and pregnancy outcomes after 96,000 embryo transfers
 Progesterone supplementation in true natural cycle FETs improves outcomes
Progesterone supplementation in true natural cycle FETs improves outcomes
 Meta-analysis finds no difference in pregnancy outcomes when using the ERA
Meta-analysis finds no difference in pregnancy outcomes when using the ERA
 RCT finds no change in birth rates for standard or ERA-timed euploid transfer
RCT finds no change in birth rates for standard or ERA-timed euploid transfer
 Meta-analysis examines impact of small fibroids on pregnancy outcomes
Meta-analysis examines impact of small fibroids on pregnancy outcomes
 Increases in immune cells associated with reduced risk of miscarriage
Increases in immune cells associated with reduced risk of miscarriage