
Researchers in a 2024 study compared pregnancy outcomes for PGT-A tested euploid embryos that were regraded after thawing, and found that embryos with a higher grade had improved outcomes compared to embryos with no change in grade.
Embryo grading is an effective tool to rank embryos for transfer, as embryos with a higher grade have a higher chance of implanting compared to embryos with a lower grade. For embryos that are frozen, they’re normally graded before freezing and not again after thawing, although they could change grade. It’s not clear if embryos that have differences in grading after thaw show differences in their ability to implant.
This study compared euploid embryos with differences in grading before and after thaw, along with euploids that didn’t re-expand after thawing. Re-expansion is an important indicator of the health and viability of the blastocyst. Blastocysts have an inner cavity called a blastocoel that is filled with water, and when they’re frozen they’re often collapsed/compacted (shrunken — the water has left the cavity!). After thawing, the blastocyst usually re-expands by taking up water and becomes full.
You can read more about re-expansion, and about embryo quality in general, in my Complete guide to embryo grading and success rates.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This was a retrospective study that took place at a single IVF center in the US between 2016 and 2022.
- Inclusions: a single euploid transfer, medicated FET. Multiple cycles per patient were permitted.
- Exclusions: Donor eggs, gestational carriers, rebiopsied embryos, mosaic embryos, Asherman’s syndrome, uterine malformations, uterine fibroids and recurrent pregnancy loss.
- A “decision support tool” was used to score embryos and rank them for transfer, which was based on the day of biopsy (5 or 6), expansion (4-6) and the embryo’s grade (A-C for the ICM or trophectoderm). Embryos were still graded by an embryologist. This tool helps to remove the subjectivity in choosing an embryo to transfer, and a previous study found this algorithm was more effective than an embryologist in choosing a high quality embryo to transfer.
- Embryos were graded at the time of biopsy and freezing, and then again after thawing at the time of transfer.
- NGS was used for PGT-A with multiple labs. Limitation as labs could give different results.
- The primary outcome was the live birth rate.
In terms of sample size, there were 4,613 patients with a total of 7,750 euploid transfers. The euploids were grouped based on whether or not their score (ie. grade) changed after thaw:
- No change in score after thaw: 5,331 euploids.
- Higher score after thaw: 486 euploids.
- Lower score after thaw: 1,726 euploids.
- No re-expansion after thaw: 207 euploids. Note that this group couldn’t be regraded because the embryo didn’t re-expand, but they were still transferred.
In terms of baseline characteristics between the groups, there was a difference in maternal age (range was 35.4 to 36.1) and AMH (3.0 to 3.5 ng/ml). There were no differences in BMI, endometrial thickness or time from embryo thaw to transfer (about 4.5 hours). Multivariate logistic regression was used to control for maternal age, AMH, BMI, endometrial thickness, year of embryo transfer, time from thaw to final embryo grading, and embryo score at time of freezing (based on the decision support tool).
Embryos regraded after thaw show differences in pregnancy outcomes
In this study, there were four groups based on how embryo grades changed after thaw. Note that they used a “decision support tool” to create a score for embryos that incorporated the day of the blastocyst, its expansion grade and its ICM and trophectoderm grade. To keep things simple, I’m just referring to a change in grade in this article, but they’re really measuring a change in the embryo’s score.
- No change in grade (score) after thaw
- Higher grade after thaw
- Lower grade after thaw
- No re-expansion after thaw
You can see the unadjusted results for clinical pregnancy rates (p< 0.0001), pregnancy loss rates (p= 0.079) and live birth rates below (p< 0.0001).
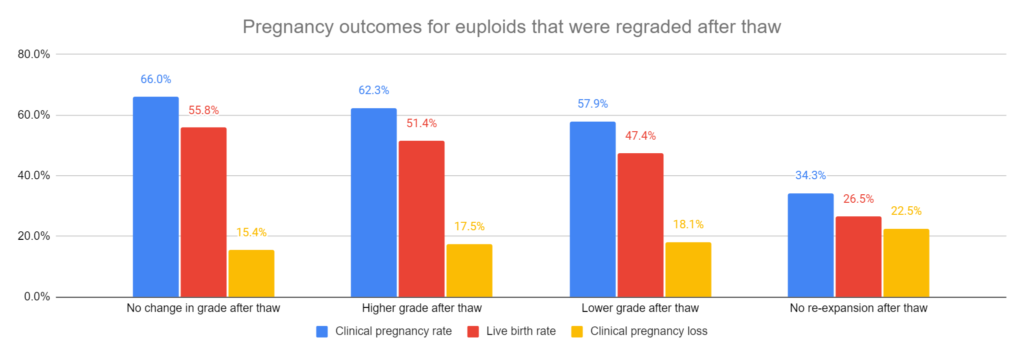
Note that these results contain all the patients with different ages, AMH levels, etc. These factors (aka confounders) could change the results, so they needed to statistically adjust the data to control for them. Take special note of the live birth rate for euploids with a higher grade after thaw vs no change in grade: 51.4% vs 55.8%. This raw data suggests that a higher grade after thaw results in a lower live birth rate, but as we’ll see below, after statistical adjustment the higher grade group has a higher odds of live birth vs the no change group.
For live birth rate (after statistical adjustment):
- Increase in live birth with higher grade after thaw vs no change in grade (51.4% vs 55.8%, odds ratio [95% CI]: 1.42 [1.14-1.76]). This means that after statistical adjustment, the odds of live birth for the higher grade group was 1.42 times (or 42% higher than) the group with no change in grade.
- Decrease in live birth with lower grade after thaw vs no change in grade (47.4% vs 55.8%, odds ratio [95% CI]: 0.70 [0.62-0.79]). This means that after statistical adjustment, the odds of live birth for the lower grade group was 0.70 times (or 30% lower than) the group with no change in grade.
- Decrease in live birth with no re-expansion after thaw vs no change in grade (26.5% vs 55.8%, odds ratio [95% CI]: 0.36 [0.26-0.51]). This means that after statistical adjustment, the odds of live birth for the lower grade group was 0.36 times (or 64% lower than) the group with no change in grade.
For clinical pregnancy rates (after statistical adjustment):
- Increase in clinical pregnancy with higher grade after thaw vs no change in grade (62.3% vs 66.0%, odds ratio [95% CI]: 1.43 [1.13-1.79]).
- Decrease in live birth with lower grade after thaw vs no change in grade (57.9% vs 66.0%, odds ratio [95% CI]: 0.71 [0.63-0.80]).
- Decrease in live birth with no re-expansion after thaw vs no change in grade (34.3% vs 66.0%, odds ratio [95% CI]: 0.35 [0.25-0.48]).
There were no differences in pregnancy loss between any of the groups compared to the no change in grade group after statistical adjustment.
Conclusions
This study found that euploids that had changed grades had different pregnancy outcomes compared to euploids that didn’t change grades.
Euploids with a higher grade after thaw were more likely to lead to a live birth, while those with a lower grade were less likely.
Euploids that didn’t re-expand after thaw had the lowest chance of live birth.
There were similar results with clinical pregnancy rates, and there were no differences in pregnancy loss rates in any of the groups.
This shows that the embryo grade after thaw matters, so maybe clinics should start grading embryos before and after thaw?
The researchers note that embryo freezing and thawing might act as a “stress test,” and embryos that are downgraded might have an inherently lower ability to implant.
I appreciate that they used euploid embryos in this study to help control for embryo quality to some degree, along with maternal age. Older women tend to show decreases in their ability to produce euploid embryos (read more about that here), so by using euploids the impact of age is reduced.
Some embryos don’t change grade after thaw, while others do, so why is this?
I think that embryologist technique is important to consider here. Embryologists can have different experience levels in biopsy, freezing and thawing. It’s possible that embryologists with less experience may be more likely to damage embryos during biopsy, and this could change the grade. As far as I can tell, this wasn’t investigated in this study and the skill level/number of embryologists is unknown; however, I’m assuming the embryologists are all well-trained. Another limitation is that they used different PGT-A labs, which have been shown to produce different outcomes.
Embryologists are also notorious for grading embryos differently (read more here), as the process is very subjective, and this could lead to differences in grading. The researchers noted that the embryologist that regraded the embryo after thaw was different 98.2% of the time from the embryologist that graded it before freezing. In a real-world situation this would be typical, but it would be nice if they used the same embryologist to keep things consistent. Once AI begins to be implemented in the lab more, I think grading embryos will be more consistent and we’ll start getting better data from studies like this.
Previous studies agree with this study, and have found that the grade of the embryo after thaw is important, as well as re-expansion (references below).
Related studies
To learn more about this topic, you can check out a number of studies referenced in this study below (5 links):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete Guide to Embryo Grading and Success Rates
Complete Guide to Embryo Grading and Success Rates
 Day 3 or Day 5 embryo transfer?
Day 3 or Day 5 embryo transfer?
 Study examines transferring a good and poor quality embryo together
Study examines transferring a good and poor quality embryo together
 Transferring a good and poor quality embryo together: a meta-analysis
Transferring a good and poor quality embryo together: a meta-analysis
 AI model predicts live births from blastocyst images with highest accuracy yet
AI model predicts live births from blastocyst images with highest accuracy yet
 Study examines association with embryo quality and male to female sex ratio
Study examines association with embryo quality and male to female sex ratio
 Study evaluates the potential of day 4, 5, 6 and 7 blastocysts
Study evaluates the potential of day 4, 5, 6 and 7 blastocysts
 Poor quality blastocysts show acceptable live birth rates, no change in perinatal outcomes
Poor quality blastocysts show acceptable live birth rates, no change in perinatal outcomes