A 2024 meta-analysis combined the results of 12 studies comparing the use of artificial oocyte activation (AOA) on IVF outcomes. They found that there were increases in fertilization and live birth rates, but only in patients with a history of fertilization problems.
When a sperm enters an egg, calcium ions are released. These calcium ions trigger the egg’s mitochondria to make energy. This is called oocyte activation and is needed for successful fertilization.
In cases of total fertilization failure, or even in cases of low fertilization, oocyte activation might be blocked. This can be corrected by artificial oocyte activation (AOA), usually by using chemicals called “calcium ionophores” that help carry calcium into the egg (shown below):
To learn more about fertilization, check my post on Abnormal fertilization.
AOA is often used in cases of no or low fertilization, but is sometimes used in patients without fertilization problems as a way to potentially prevent embryo arrest. Embryo arrest is when embryos stop developing during the cleavage stage — to learn more, check out my post on Embryo arrest.
This post is a summary of a meta-analysis by Zhang et al. (2024), who combined the results of 12 studies investigating the use of AOA for patients with or without fertilization problems. Patients with fertilization problems had a history of <50% fertilization, and those without fertilization problems had a history of embryo arrest or male factor.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- Only studies that used calcium ionophores A23187 or ionomycin were included, in randomized or non-randomized controlled trials. Only ICSI.
- Studies were excluded if they focused on patients with a specific diagnosis, like advanced maternal age, PCOS or some forms of teratozoospermia.
- The primary outcome was the fertilization rate and the live birth rate.
- AOA was typically performed by adding the inseminated eggs to culture media containing the ionophore for about 15 minutes after ICSI. Different timings and concentrations of the ionophore were used between the studies.
Artificial oocyte activation improves fertilization and live birth rates
Among the 12 studies in this meta-analysis, involving patients with or without fertilization problems:
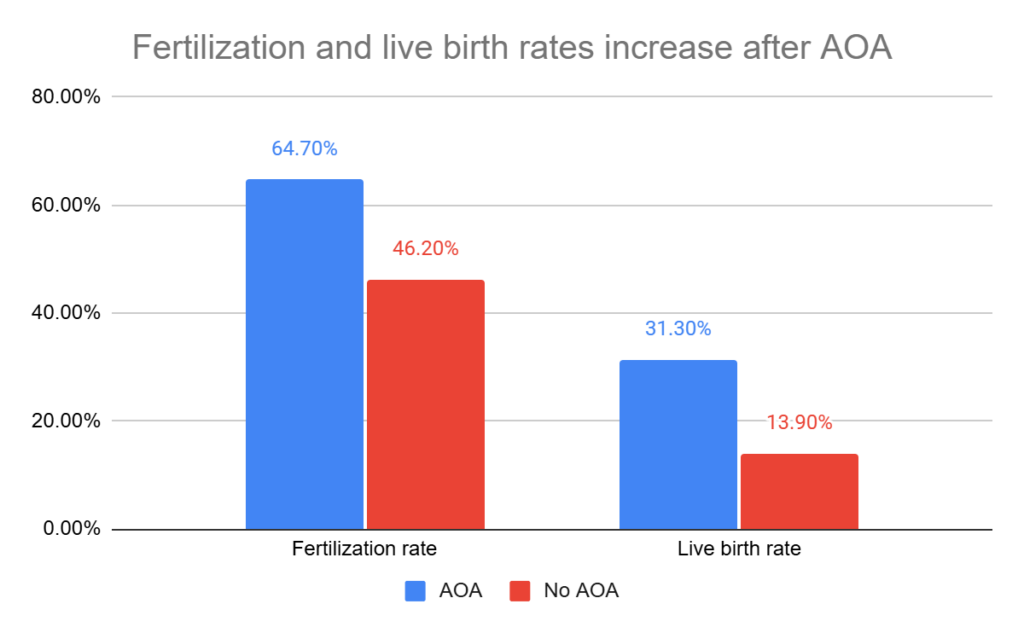
- AOA improved the odds of fertilization by about 2 times (64.7% vs 46.2%, odds ratio 1.99, 95% CI: 1.16-3.41, 12 studies, 16,804 patients, I2= 98%). This is a very large I2 value, indicating a very high amount of variability between the studies.
- AOA improved the odds of live birth by about 4.5 times (31.3% vs 13.9%, odds ratio 4.58, 95% CI: 1.52-13.80, 8 studies, 1268 patients, I2= 85%).
Next, they looked at outcomes for patients with or without fertilization problems.
- In patients with fertilization problems (history of <50% fertilization), AOA improved the odds of fertilization by about 3 times (63.1% vs 34.0%; odds ratio 3.19, 95% CI: 1.62-6.28, 7 studies, 7102 patients, I2= 98%).
- In patients with fertilization problems (history of <50% fertilization), AOA improved the odds of live birth by about 11 times (30.1% vs 3.40%; odds ratio 11.15, 95% CI: 2.96-41.97, 4 studies, 636 patients, I2= 52%).
- In patients without fertilization problems (history of embryo arrest/male factor), AOA didn’t improve the odds of fertilization (5 studies, 6450 patients, I2= 82%).
- In patients without fertilization problems (history of embryo arrest/male factor), AOA didn’t improve the odds of live birth (4 studies, 632 patients, I2= 85%).
This tells us that the benefits of AOA are really only seen in patients with a history of fertilization problems.
Artificial oocyte activation ineffective for overcoming embryo arrest
Besides fertilization and live birth rates, which were the primary outcome, the researchers also compared a number of different IVF and pregnancy outcomes.
In patients with fertilization problems (history of <50% fertilization):
- AOA improved the blastocyst formation rate by about 1.4 times (odds ratio 1.35, 95% CI: 1.04-1.75).
- AOA improved the clinical pregnancy rate by about 3.8 times (odds ratio 3.75, 95% CI: 1.63-8.65).
In patients without fertilization problems (history of embryo arrest/male factor):
- AOA didn’t improve any of the outcomes examined (rates for blastocyst formation, high quality blastocysts, clinical pregnancy).
AOA improved fertilization rates in patients with fertilization problems, which increased the number of fertilized eggs that could become blastocysts. The patients without fertilization problems, who had a history of embryo arrest or male factor, didn’t see any increase in the number of blastocysts. This suggests that AOA isn’t effective for overcoming embryo arrest.
No safety concerns with artificial oocyte activation
The authors note that AOA didn’t seem to cause any safety concerns. Studies showed no increased risk of adverse outcomes like miscarriage, egg degeneration (death), preterm delivery, gestational age, birth weight, congenital abnormality and major birth defects.
Conclusions
When looking at all the data, using AOA helped increase the rates of fertilization and live birth.
However, when breaking down the studies, only patients with fertilization issues saw improvements in fertilization and live birth. Patients who didn’t have fertilization problems didn’t see any benefit from using AOA.
The studies also checked other results, like how well AOA helped form blastocysts. Again, only patients with fertilization problems saw improvements. This suggests that AOA isn’t effective for overcoming embryo arrest problems.
According to the studies, using AOA was safe. There were no increases in miscarriages or preterm births.
The authors pointed to research that shows AOA had a negative effect on live birth rates in patients with certain types of male factor, suggesting that AOA may be detrimental for some patient groups. Additionally, prolonged exposure to calcium ions in AOA can disrupt cell balance and gene activity, raising concerns about its long-term effects on embryo health and development. There is limited follow-up on children born after AOA, but the studies that have been done have shown no impact on neurodevelopmental and language outcomes.
The authors note that AOA should be “strictly limited to patients with appropriate indications” and that any children born from this technique should be closely monitored. More high quality studies (RCTs) are needed to evaluate its effectiveness.
There was significant variability between the studies (the reason for the high I2 values). This is due to the studies having different patient characteristics and treatment protocols. There is a lack of consistency in how AOA is used.
Related studies
To learn more about this topic, you can check out a number of studies referenced in this study below (14 links, including the studies included in the meta-analysis):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Artificial oocyte activation improves IVF outcomes in clinical trial
Artificial oocyte activation improves IVF outcomes in clinical trial
 Embryo Arrest
Embryo Arrest
 Study compares IVF outcomes by follicle size
Study compares IVF outcomes by follicle size
 Sleep quality and its impact on IVF outcomes
Sleep quality and its impact on IVF outcomes
 Can sperm and egg be “genetically incompatible”?
Can sperm and egg be “genetically incompatible”?
 Pilot study shows improved IVF outcomes after spindle transfer in women with poor egg quality
Pilot study shows improved IVF outcomes after spindle transfer in women with poor egg quality
 Mini “MRI” reads embryo metabolism to help pick the best embryo for IVF
Mini “MRI” reads embryo metabolism to help pick the best embryo for IVF
 Sperm DNA fragmentation associated with lower embryo quality and implantation
Sperm DNA fragmentation associated with lower embryo quality and implantation