
Researchers in their 2022 Cochrane review, performed a meta-analysis and combined the results of 32 studies that compared pregnancy outcomes of blastocyst and cleavage stage embryos, and found that blastocysts tend to produce better outcomes.
Embryos can be transferred during the cleavage stage (days 2-3) or during the blastocyst stage (days 5-7). Embryos can arrest between day 3 and day 5, which acts as a filter for embryos with low implantation potential. However, it isn’t clear if blastocysts outperform cleavage stage embryos, and whether or not certain patients benefit more from a particular embryo type.
Glujovsky et al. (2022) performed a systematic review and meta-analysis and combined the results of 32 randomized controlled trials (RCTs) that compared pregnancy outcomes for blastocyst or cleavage stage embryo transfers. A total of 5,821 participants were included in the 32 RCTs.
Update (2026): A newer Cochrane update including 36 RCTs and 8,389 women found similar results. Blastocyst transfer likely improves live birth per fresh transfer and may slightly increase cumulative live birth within 12 months, but also increases preterm birth risk and cycle cancellation. Most data remain from good prognosis patients.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- Blastocysts were day 5 or 6, cleavage stage were day 2 or 3.
- Conventional IVF or ICSI was performed.
- No in vitro maturation, PGT-A or donor egg cycles.
- These were all fresh transfers, except for studies that measured cumulative pregnancy rates.
- Different numbers of embryos were transferred among the studies.
- Different criteria was used for choosing embryos of sufficient quality to transfer.
- Different media was used to culture the embryos.
- When freezing was done, different methods of freezing were performed.
- The average age was 29 to 34, and most studies recruited women <40.
- Most studies used similar ovarian stimulation protocols.
I put those 4 points in bold because they’re limitations of the meta-analysis, but this is the state of the RCTs available and obviously better studies need to be done.
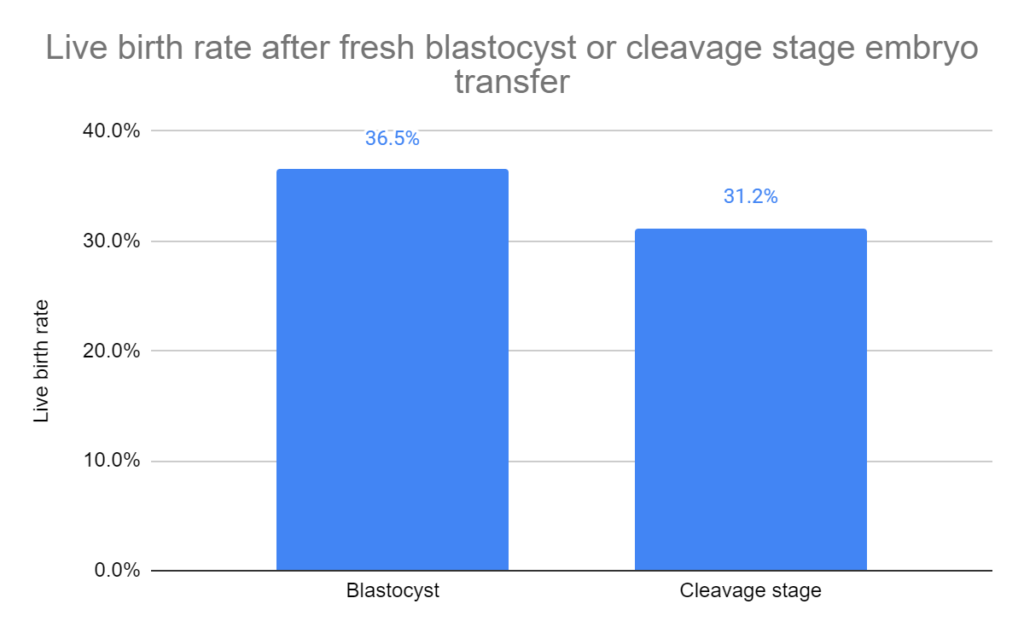
Live birth rates for blastocyst vs cleavage stage transfer
Live birth rates were higher for patients who transferred blastocysts vs cleavage stage embryos (36.5% vs 31.2%, odds ratio [95% CI]: 1.27 [1.06-1.51], moderate heterogeneity I2 = 53%; 15 studies, 2,219 participants). The quality of evidence was indicated as low.
They then took these studies and performed different subgroup analyses.
Subgroup analysis for the number of embryos transferred. They found an increase in live birth rates for blastocysts when more cleavage stage embryos were transferred vs blastocyst. When a single embryo was transferred, or when equal numbers were transferred, there was no statistical difference.
Subgroup analysis for the prognosis. In good prognosis patients, there was an increase in live births when transferring blastocysts vs cleavage stage embryos. There was no statistical difference in poor prognosis patients.

Clinical pregnancy rates for blastocysts vs cleavage stage transfer
Clinical pregnancy rates were higher for patients who transferred blastocysts vs cleavage stage embryos (44.0% vs 39.0%, odds ratio [95% CI]: 1.25 [1.12-1.39], moderate heterogeneity I2 = 51%; 32 studies, 5,821 participants). The quality of evidence was indicated as moderate.

They then took these studies and performed different subgroup analyses.
Subgroup analysis for the number of embryos transferred. They found an increase in clinical pregnancy rates for blastocysts when an equal number, or a single embryo was transferred. When more cleavage stage than blastocysts were transferred, there was no statistical difference.
Subgroup analysis for the prognosis. In good prognosis patients, there was an increase in clinical pregnancies when transferring blastocysts vs cleavage stage embryos. There was no statistical difference in poor prognosis patients.

Cumulative clinical pregnancy rates for blastocyst vs cleavage stage transfer
Now that we’ve seen what the live birth and clinical pregnancy rates look like with blastocyst vs cleavage stage transfer, let’s turn our attention to the cumulative pregnancy rate.
The cumulative pregnancy rate is often considered a better measure of success, because it includes multiple embryo transfers and is more similar to what patients do in real life.
For the cumulative pregnancy rate, we might be looking at a sequence where a patient transfers their first embryo fresh, then follows it up with one or more frozen transfers if the fresh fails. The cumulative pregnancy rate accounts for pregnancies that occur at any point in this sequence.
There was no statistical difference in cumulative clinical pregnancy rates for patients who transferred blastocysts vs cleavage stage embryos (48.9% vs 52.1%, odds ratio [95% CI]: 0.89 [0.64-1.22], high heterogeneity I2 = 71%; 5 studies, 632 participants). The quality of evidence was indicated as very low.
They then took these studies and performed different subgroup analyses.
Subgroup analysis for the number of embryos transferred. They found no statistical differences in cumulative clinical pregnancy rates for patients who had a single embryo transferred or an equal number of blastocysts and cleavage stage embryos.
Subgroup analysis for the prognosis. They found improved cumulative pregnancy rates in good prognosis patients who transferred cleavage stage embryos vs blastocysts. The studies didn’t look at poor prognosis.
Subgroup analysis for freezing method. They found improved cumulative pregnancy rates for cleavage stage transfers when slow freezing was used, and improved rates for blastocyst transfers when vitrification was used. Slow freezing is an older method of freezing, while vitrification is the standard these days.

Miscarriage rates for blastocyst vs cleavage stage transfer
There was no statistical difference in miscarriage rates for patients who transferred blastocysts vs cleavage stage embryos (8.2% vs 6.7%, odds ratio [95% CI]: 1.24 [0.98-1.57], no heterogeneity I2 = 0%; 21 studies, 4,106 participants). The quality of evidence was indicated as low.
Number of cancelled transfer cycles for blastocyst vs cleavage stage embryos
As embryos develop from day 3 to day 5, many may arrest or stop developing, leading to cancelled transfer cycles.
There was a statistically significant decrease in the rates of no-transfer cycles for patients who transferred blastocysts vs cleavage stage embryos (8.5% vs 3.6%, odds ratio [95% CI]: 2.50 [1.76-3.55], low heterogeneity I2 = 36%; 17 studies, 2,577 participants). The quality of evidence was indicated as moderate.
Conclusions
This study found that clinical pregnancy and live birth rates were higher for blastocyst transfers. This was also true for good prognosis patients, but there was no difference in poor prognosis patients.
Cumulative pregnancy rates were similar for blastocyst and cleavage stage transfers. Miscarriage rates were also similar.
One analysis looked at the freezing method performed. Slow freezing was the standard method in the past, while vitrification is more common these days. Limited evidence shows that cleavage stage embryos have higher cumulative pregnancy rates when slow freezing was used, but blastocysts performed better when vitrification was used.
In general, the studies in this meta-analysis were pretty variable. This was due to differences in the number of embryos transferred, culture media used, freezing method and selection policy for transferring embryos of a certain quality.
Many studies involved transferring more cleavage stage embryos than blastocysts. Subgroup analyses that assessed single or equal embryo transfers found no difference for live birth or cumulative pregnancy rates, but clinical pregnancy rates were higher with blastocyst transfers.
The researchers found no evidence of publication bias among the studies used in this meta-analysis. However, they note that 6 RCTs are in progress, all of which started more than 5 years ago without any data published as of 2022, suggesting possible publication bias for these studies. In other words, the researchers for those particular studies may have issues with their results and have chosen not to publish.
The authors state that more studies are needed, particularly those that use single embryo transfers, examine poor prognosis patients, and measure cumulative pregnancy rates with vitrification as a freezing method.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete Guide to Embryo Grading and Success Rates
Complete Guide to Embryo Grading and Success Rates
 Day 3 or Day 5 embryo transfer?
Day 3 or Day 5 embryo transfer?
 Increased risk factors with blastocyst transfer vs cleavage stage
Increased risk factors with blastocyst transfer vs cleavage stage
 Predicting how many day 3 embryos make it to blastocyst
Predicting how many day 3 embryos make it to blastocyst
 Predicting live birth rates, multiples based on 223,377 transfers
Predicting live birth rates, multiples based on 223,377 transfers
 Age-specific blastocyst conversion rates and other IVF outcomes in good prognosis women
Age-specific blastocyst conversion rates and other IVF outcomes in good prognosis women
 Fewer embryos give better results when transferred on day 3, not day 5
Fewer embryos give better results when transferred on day 3, not day 5
 Initial and doubling beta-hCG linked to embryo development and quality
Initial and doubling beta-hCG linked to embryo development and quality