
This post discusses the use of supplements to improve egg quality for IVF success, exploring the supporting evidence for a range of supplements like N-acetyl-cysteine, Melatonin, L-arginine, Myo-inositol, CoQ10, L-carnitine, DHEA, folic acid/folate, and vitamins E, C, D, and B.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Table of Contents
What are supplements?
Supplements can be:
- Vitamins
- Minerals
- Herbs
- Amino acids
- Antioxidants
In the USA, supplements are classified as food and not as drugs. This means that supplements aren’t regulated the same way as drugs and don’t require testing before being sold to the public.
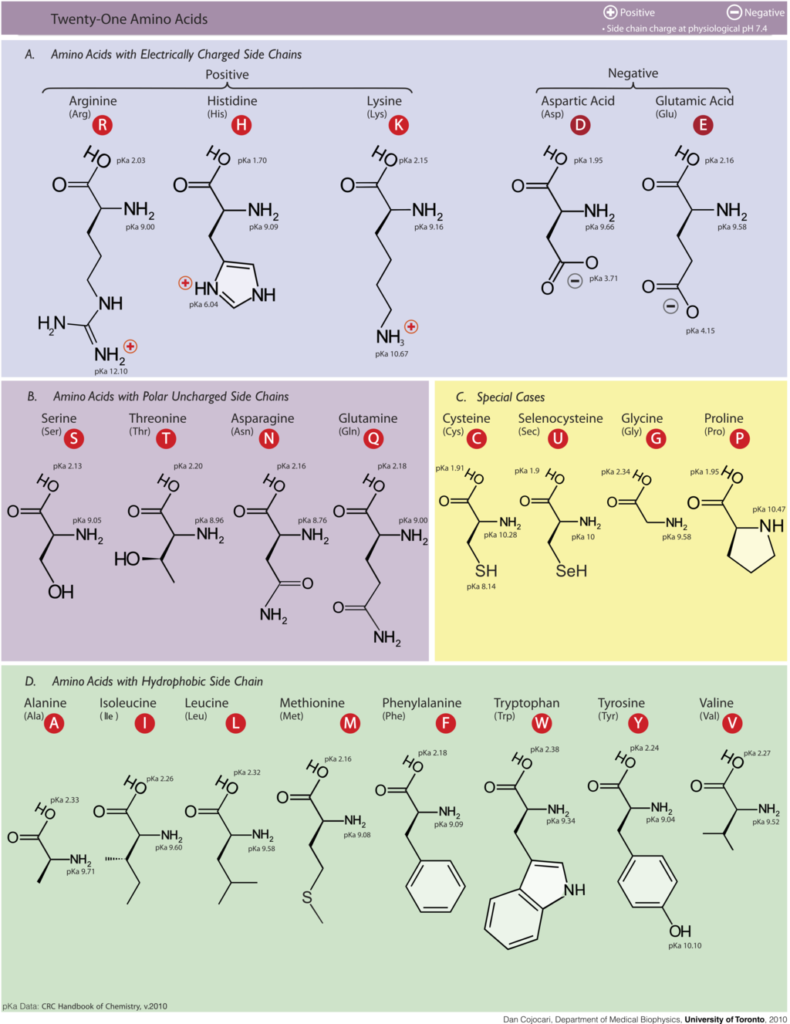
Amino acids
Our body is made up of proteins. Not the dietary kind (although these are proteins too), but biochemical proteins that can make enzymes, cell receptors, and all basically every part of a cell and your body that you can think of.
These proteins are big molecules that are made up of building blocks called amino acids. There’s 20 amino acids in our body and they’re the alphabet for protein synthesis.
{kind=link}
Our body can make many amino acids on its own, but some need to be supplemented through the diet. Supplementing with certain amino acids may be helpful for fertility.
Vitamins
Vitamins, or coenzymes, are special molecules that help enzymes in the cell (or egg) do their job.
We can produce some vitamins ourselves (vitamin D for example), but many need to be supplemented from our diet. Here’s what some common vitamins look like:

Antioxidants
Reactive oxygen species (ROS) are highly reactive molecules that can cause damage to DNA or other molecules. They can be produced by normal cellular metabolism or by introducing them through lifestyle choices (smoking, drinking, diet, etc.). In low levels they serve a necessary purpose for the cell to function, but when ROS levels increase this can lead to “oxidative stress.”
With all these highly reactive ROS molecules floating around, they can cause some serious damage that results in lower egg or embryo quality and can impact implantation.
Antioxidants work against ROS by “scavenging” them.
Antioxidants are an easier target for ROS than DNA (for example) – so ROS will preferentially react with the antioxidant. Once it reacts, it’s no longer a ROS. So antioxidants drive ROS levels down – reducing oxidative stress!
The balance of ROS and antioxidants is important.
Our cells have a lot of antioxidants that are made by the cell to maintain this balance. Diet and lifestyle choices can impact the balance of ROS and antioxidants. Cigarette smoke, for example, contains lots of ROS which can damage DNA and lead to mutations and possibly cancer (Becker et al. 2014).
How long does it take for supplements to work to improve egg quality?
To get a sense for how long it takes, we need to better understand how follicles and eggs develop.
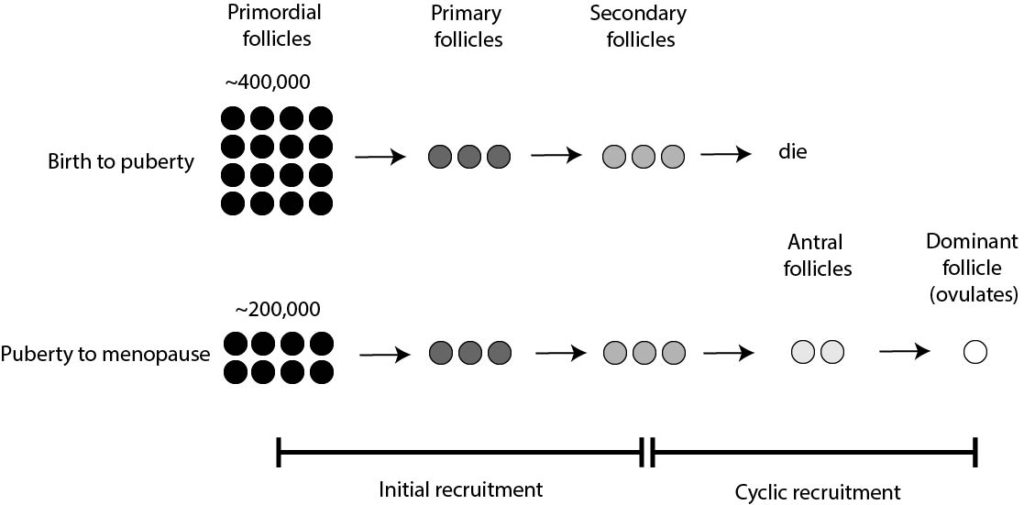
You are born with all the eggs you’ll have. These eggs are actually follicles called primordial follicles and represent your ovarian reserve.
At 20 weeks gestation, you had about 6-7 million primordial follicles each containing an immature egg. By birth, you had about 300k-400k remaining. This reduction is due to a process called initial recruitment:
- Some of these primordial follicles go on and develop into primary follicles
- These primary follicles go on to develop into secondary follicles
- These secondary follicles die.
This process continues until puberty, when you have about 200k primordial follicles left, and your body begins to produce hormones. Lots of them!
In response to these hormones, secondary follicles (from initial recruitment) can develop into antral follicles. These can then go on to produce a dominant follicle containing a mature egg for ovulation. This happens every month and is called cyclic recruitment.
In terms of timing (McGee 2000):
- Primordial follicle to Primary follicle: unknown
- Primary follicle to Secondary follicle: at least 120 days
- Secondary follicle to Antral follicle: 71 days
- Antral follicle to Dominant follicle (ovulates): 14 days
- 120+71+14 =205 days + however long it took for the primordial follicle to make the primary follicle.
In short, egg development takes awhile.
Most will recommend 90 days, which covers the Secondary follicle to Dominant follicle stages. I’m not sure if this is sufficient and I can’t find any information to confirm this.
If a study reports a benefit of a supplement, it’s probably best to follow their dosage/timing and whatever your doctor recommends.
Egg quality supplements and success rates
Overview
Here I’ll present evidence from a Cochrane review (Showell et al. 2020), which is a meta-analysis that combines the results of multiple high quality studies (randomized controlled trials or RCTs).
There is a ton of data in the report, and for simplicity I’m only going to report on the clinical pregnancy data used in women who were attempting natural conception or using assisted reproduction (including IUIs, IVF and ICSI).
If you’d like to look at all the data from this study (including data on live birth rates, adverse events, IVF/ICSI), you can check out this post:
Type of supplement:
- N-acetyl-cysteine*: increased pregnancy rates (8 RCTs, 1,590 women)
- Melatonin*: increased pregnancy rates (7 RCTs, 678 women)
- Vitamin E : no difference in pregnancy rates (1 RCT, 103 women)
- Vitamin C : no difference in pregnancy rates (2 RCTs, 899 women)
- L-arginine : no difference in pregnancy rates (2 RCTs, 71 women)
- Vitamin D : no difference in pregnancy rates (1 RCT, 52 women)
- Vitamin B : no difference in pregnancy rates (1 RCT, 102 women)
- Myo-inositol + folic acid : no difference in pregnancy rates (1 RCT, 94 women)
- CoQ10*: increased pregnancy rates (4 RCTs, 397 women)
- L-carnitine*: increased pregnancy rates (2 RCTs, 450 women)
- Note that N-acetyl-cysteine and L-carnitine both had significant heterogeneity (variability) in their studies, so it’s less clear if these are effective.
- Note that the quality of evidence is indicated as LOW for these studies (discussed below).
*Described in more detail below.
Diagnosis:
- PCOS: increased pregnancy rates (15 RCTs, 1,908 women)
- Unexplained fertility: no difference in pregnancy rates (4 RCTs, 997 women)
- Tubal: no difference in pregnancy rates (2 RCTs, 71 women)
- Poor responders: no difference in pregnancy rates (1 RCT, 65 women)
- Poor ovarian reserve: no difference in pregnancy rates (2 RCTs, 266 women)
- Endometriosis: no difference in pregnancy rates (1 RCT, 280 women)
Adverse events:
- Miscarriage: no difference (24 RCTs, 3,229 women)
- Multiple pregnancy: no difference (9 RCTs, 1,886 women)
- Ectopic pregnancy: no difference (7 RCTs, 308 women)
- Preterm birth: no difference (2 RCTs, 220 women)
- Placenta previa: no differences (1 RCT, 180 women)
- Preeclampsia: no difference (1 RCT, 160 women)
N-acetyl-cysteine (NAC)
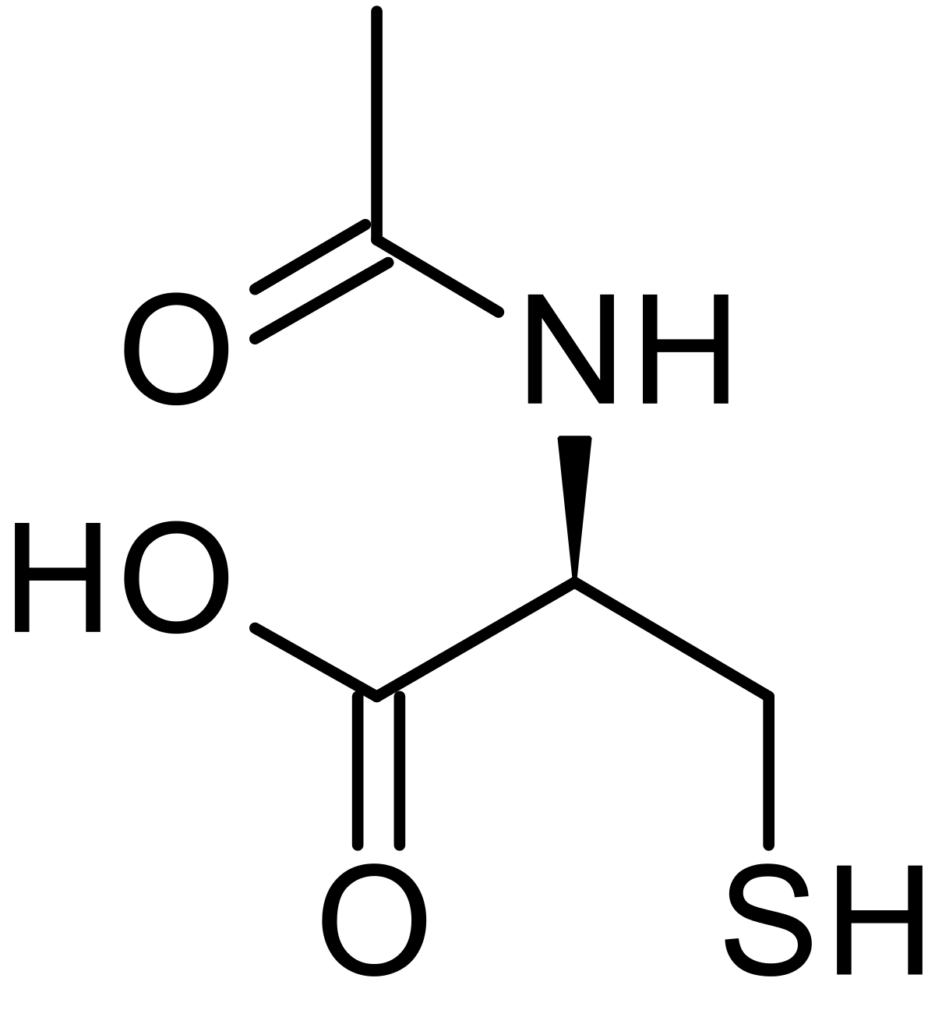
NAC is a medication that can be used to treat Tylenol (acetaminophen) overdoses by increasing levels of the antioxidant glutathione. It’s sometimes used as a supplement, although it’s been banned for this purpose in the US as of 2021.
Here’s some more information regarding the patients and dosage on a couple of the studies from Showell et al. 2020:
- Ovulation induction study with clomid (400 patients)
- 1,200 mg/day of NAC for 5 days starting on CD2
- Ovulation induction study with letrozole (130 PCOS patients)
- 1,200 mg/day of NAC for 5 days starting on CD3
Melatonin
Melatonin is a natural hormone that regulates our sleep-wake cycles. It also plays a role as an antioxidant.
Here’s some more information regarding the patients and dosage on a couple of the studies from Showell et al. 2020:
- IVF study (80 women with DOR)
- 3 mg capsule every night, starting 5 days before ovarian stimulation start
- IUI study (198 PCOS patients)
- 3 mg tablet from CD3 to hCG trigger
Coenzyme Q10 (CoQ10)
Coenzyme Q10 (or CoQ10 for short) is an antioxidant that also plays a role in producing energy for the cell in the mitochondria.
With older age, CoQ10 levels decrease, so we can see why CoQ10 might be an important supplement in improving egg quality.
In studies, CoQ10 has lead to more mature oocytes, increased embryo quality, and better response in women with DOR; 600 mg/day seems to be the standard dose (Giannubilo 2018).
As described in the Cochrane review above, 7 RCTs showed a positive impact of CoQ10 on pregnancy rates (Showell et al. 2020), here’s more details on two of them:
- IVF/ICSI (39 women total, RCT)
- 600 mg CoQ10 1x/day for 2 months before IVF
- Pregnancy rate: 35.2% (with CoQ10) vs 27.2% (without CoQ10)
- PCOS women, timed intercourse (101 women total, RCT)
- 60 mg CoQ10 3x/day + 150 mg of clomiphene for 5 days/cycle for 2-3 cycles
- Pregnancy rate: 34.5% (with CoQ10) vs 5.4% (without CoQ10)
L-carnitine
Carnitine is an antioxidant that is made from lysine (an amino acid) and you can find lots of it in meat. It plays a role in producing energy in the mitochondria, reducing oxidative stress, and reducing membrane damage to the mitochondria. Various studies have shown that it has a positive impact on fertility (reviewed by Agarwal 2018):
- Improves disorders like PCOS and endometriosis
- Increases gonadotropins and oocyte quality
As shown above, the Cochrane review (Showell et al. 2020) found an increase in pregnancy rates. Here’s some details from one of the studies (Ismail 2014):
- PCOS women, timed intercourse (170 women total, RCT)
- 3 g/day L-carnitine (day 3 of cycle until pregnant) + 250 mg clomiphene (day 3-7 of cycle)
- Pregnancy rate: 49.4% (with carnitine) vs 1.1% (without carnitine)
DHEA
DHEA is a precursor for testosterone and estradiol and is typically supplemented in women with DOR or poor ovarian responders (PORs). It has been shown to improve response to stimulation, ovarian reserve, oocyte/embryo quality and pregnancy/live birth rates. (Chern 2018).
A 2015 Cochrane review looked at the data in PORs (Nagels 2015):
- Improved odds of live birth/ongoing pregnancy by 1.88 (8 RCTs, 878 women, moderate quality evidence). However, when another analysis was performed that removed trials at high risk of performance bias, the results weren’t significant.
- Increased odds of pregnancy by 1.34 (12 RCTs, 1246 women, moderate quality evidence)
- No difference in miscarriage rates (8 RCTs, 950 women, moderate quality evidence)
- Length of treatment varied from 2 to 26 weeks – no conclusion on optimal length
- Dosage varied but most common was 75 mg/day
Additionally, this Cochrane review identified two studies with women who were not PORs and found no difference in pregnancy rates. So DHEA may be beneficial only to PORs.
Folic acid (folate)
Folic acid/folate is involved in DNA and protein synthesis and plays a key role in breaking down the amino acid homocysteine. Without adequate folic acid, hyperhomocysteinemia can occur which is linked to increases in miscarriage and neural tube defects in the fetus (Carrell 2015).
Based on a review by Carrell (2015), studies show:
- Higher blood folate levels correlate with better embryo quality and pregnancy rates
- Increased homocysteine levels (=low folate) correlate with lower embryo quality
- Higher implantation, pregnancy and live birth
- Although there’s mixed data: some studies show no benefit for pregnancy or live birth.
Recommended dose is 400 ug/day, though one study showed higher success with 800 ug/day (Carrell 2015).
The problem with supplements
The data with supplements can be inconsistent, and this is due in part to their lack of regulation.
There are a number of problems with the supplement industry that people may not be aware of (reviewed by Starr 2015 if not referenced):
- Traditional drugs need to go through clinical trials to show they work and that they’re safe. This isn’t required for supplements. Supplements are not approved by the FDA and are not regulated like prescription or over the counter drugs.
- As long as no new supplement ingredient is being introduced, there’s no need to notify the FDA when the product is marketed. For new ingredients that haven’t been marketed as supplements before, premarketing evidence is technically required by the FDA. However, many new ingredients are not reported and are absent on the supplement label, making it difficult to identify violators.
- Supplements can contain ingredients at any concentration and in any combination, making them very inconsistent. One report found that vitamin D concentrations ranged from 9% to 146% of the stated concentration.
- Reports have found that supplements can contain contaminants, or ingredients not listed on the label. In one report, 83% of herbal products switched the active ingredient to something else.
- Manufacturers set their own standards, and the same ingredient from different manufacturers can be very different in terms of composition, strength or bioavailability.
- Monitoring for supplement safety is voluntary.
- While supplements can’t make medical claims to treat or prevent a specific disease, they can make general health claims based on evidence, however there aren’t standards for what evidence is used. These claims aren’t evaluated by the FDA.
- Because supplements aren’t regulated, and they’re cheap to make, it’s a huge industry: there were $30 billion in sales in 2011 (this has doubled in 2023). It’s driven by commercial interest and supplements are marketed with misleading language to sell, making people believe that they are just as effective as drugs (stating that they’re “clinically tested” or “doctor formulated”), or can use words like “natural” to make them seem more attractive. An investigation by the Office of Inspector General revealed that most supplement health claims are misleading, uninformative and inconsistent. In supplements that combine different ingredients, often the claims made on these products are based only on one of the ingredients, not the whole combination, which can be misleading.
Many patients take multiple supplements simultaneously, which could lead to problems. There’s evidence that different supplements can interact with each other, or with other substances, to reduce their effectiveness (Institute of Medicine, 2005). Additionally, and I’m speculating here, it’s possible that taking multiple supplements might lead to a buildup of toxic metals in the body:
- Supplements can contain trace amounts of heavy metals such as lead, mercury, arsenic and cadmium, which are often found in the soil and absorbed by plants. When supplements are manufactured using these plants or minerals, small amounts of these metals can end up in the final product.
- A study by Zhang et al. (2023) found toxic metals in six prenatal vitamin brands in the US, which were below the FDA limits at the recommended dosages. This is good, but using multiple supplements could potentially push these levels above safe limits, increasing health risks. As far as I’m aware, there’s no data confirming this by measuring toxic metals in people combining multiple supplements.
- In their umbrella review on the use of supplements for female infertility, Pandey et al. (2024) show that combining multiple supplements didn’t impact miscarriage rates, although the quality of evidence was rated as low and it doesn’t take into consideration long term effects of multiple supplement use. It’s not clear how many supplements were combined in this research (multiple micronutrients (MMN), vitacap or seidivid were listed).
So how to make sure the supplements you’re taking are safe?
According to pharmacy professor C. Michael White in his article on The Conversation, because of relaxed supplement regulations it’s up to the consumer to make sure the supplements they’re taking are safe. In some cases, manufacturers might list their own lab and its quality standards, but these labs can be biased and can give incorrect results. When purchasing dietary supplements, White recommends that consumers prioritize products verified by reputable independent labs like the United States Pharmacopeia (USP), NSF International, and ConsumerLabs.com, which test for accurate ingredient listings and safe contamination levels.
Do supplements really work?
Yes! Some do anyway – and are even encouraged by doctors (Carrell 2015):
- Folic acid (folate) for pregnancy to prevent neural tube defects in the fetus
- Iodine for pregnant/breast feeding women for hormone synthesis and fetal brain development
- Omega-3 fatty acids for fetal brain and retinal development
As far as improving egg quality with supplements? We don’t know. We don’t know if it improves egg quality, or if it harms egg quality.
The evidence from the Cochrane review (Showell et al. 2020) as shown above – is low quality (where “the true effect might be markedly different from the estimated effect”).
Why is the evidence low quality? A lot of the studies:
- Are small
- Have a high risk for bias (poor reporting/inconsistency/blinding/etc)
- Show mixed results (heterogeneity)
Often the studies aren’t even looking at the same thing:
- One study might look at PCOS patients, another at endometriosis patients
- Another might use 800 ug of folate instead of 400 ug
- Some might combine different supplements instead of just one
So it’s hard to make strong conclusions. Bigger and better studies are needed to see what works and what doesn’t.
But there really isn’t any incentive for manufacturers to produce quality studies, since this isn’t needed by the FDA, and they’re expensive to run. It can also hurt their reputation if the data is negative (in which case they might not even publish it anyway).
There’s a lot of anecdotes on social media about supplements that give hope to people in the same situation. Maybe it really did help those people, or maybe it was something else they did (like eat healthier, stop drinking, etc.), but without well designed studies we don’t know if it’s true for sure.

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to egg quality
Complete guide to egg quality
 Meta-analysis shows growth hormone improves endometrial function
Meta-analysis shows growth hormone improves endometrial function
 Mitochondria and egg quality
Mitochondria and egg quality
 CoQ10 and other supplements improve IVF outcomes in women with ovarian aging
CoQ10 and other supplements improve IVF outcomes in women with ovarian aging
 Meta-analysis combines 38 studies on treatments for diminished ovarian reserve
Meta-analysis combines 38 studies on treatments for diminished ovarian reserve
 Comprehensive review combines research on use of supplements for female infertility
Comprehensive review combines research on use of supplements for female infertility
 Egg freezing and thawing
Egg freezing and thawing
 Large trial examines impact of growth hormone on IVF success
Large trial examines impact of growth hormone on IVF success