In a 2025 study, researchers masked mosaic PGT-A results and found that mosaic reporting did not meaningfully improve embryo selection or live birth prediction beyond standard criteria, suggesting that PGT-A’s main clinical value lies in identifying clearly aneuploid embryos.
Embryos with the correct number of chromosomes are called euploid and are considered chromosomally normal. An aneuploid embryo has one or more chromosomes missing or extra, while mosaics have a mix of euploid and aneuploid cells.
Many clinics don’t transfer mosaics or discard them, but what isn’t clear is if labeling embryos as mosaic actually helps predict live birth or improves embryo selection.
A study by Gill et al. (2025) tested this question directly. Instead of reporting mosaic results to clinics, the researchers masked them until after embryo transfers and pregnancy outcomes were known. Only embryos that clearly tested as aneuploid were not transferred. All other embryos, including those with mosaic results, were transferred based on factors like embryo quality and day of biopsy.
For more background, check out my Complete guide to mosaic embryos.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- Study type: Prospective, double-blinded, multisite study with a primary US cohort (2020–2022) and an independent European validation cohort (2022–2024).
- Participants: A total of 9,828 single frozen embryo transfers from 7,564 IVF cycles in the US cohort, with an independent European validation cohort of 5,487 single embryo transfers. Included were single frozen embryo transfers of embryos reported as negative for whole-chromosome and segmental aneuploidy, from both autologous and donor cycles. Embryos tested for monogenic disorders or structural rearrangements were excluded.
- PGT-A details: All embryo biopsies were analyzed using the same next-generation sequencing platform (PGTSeq-A) at Juno Genetics. Aneuploidy was called only when both chromosome copy number and SNP-based testing confirmed aneuploidy.
- Primary outcome: Live birth rate per embryo transfer.
Overall differences were driven by a small subgroup of mosaic embryos
In this study, embryos were tested by PGT-A and all non-aneuploid embryos were transferred without clinics knowing if they were mosaic or euploid. Only after pregnancy and live birth outcomes were known did the researchers unmask the PGT-A results.
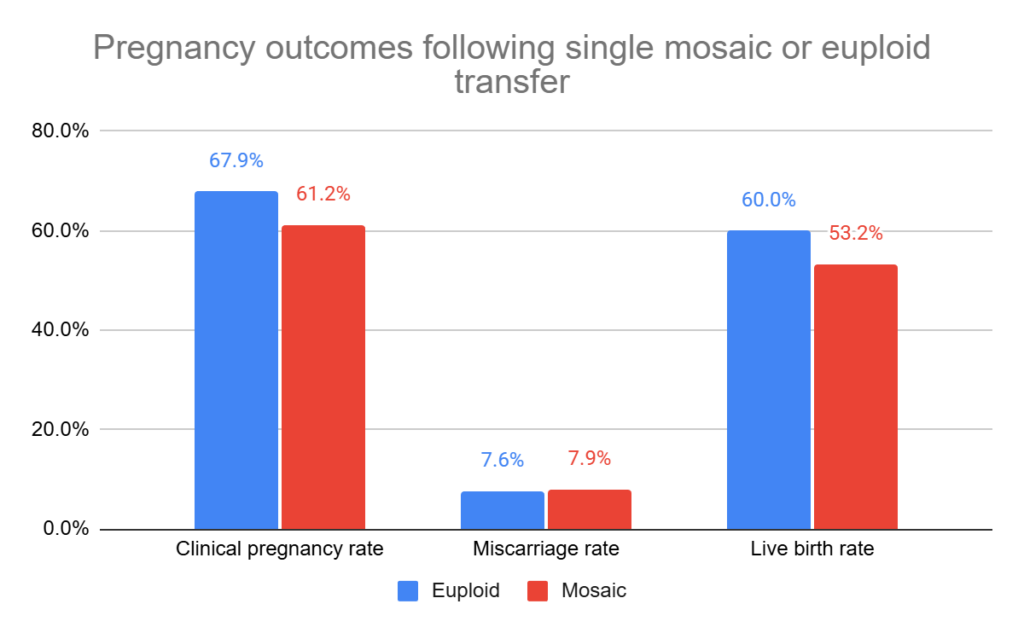
After the euploid or mosaic results were unmasked, euploid embryos had a higher live birth rate (60.2%) compared with embryos with mosaic results (60.2% vs 53.2%, adjusted odds ratio [95% CI]: 0.79 [0.70-0.89], p= 0.0001).
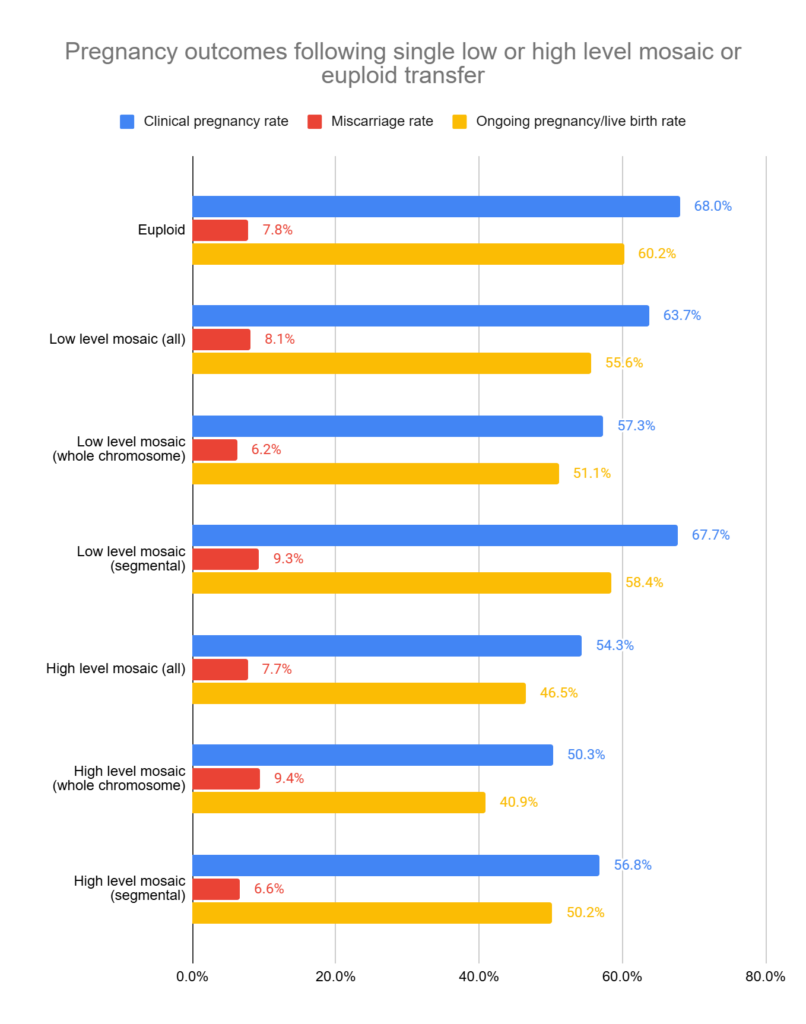
However, this difference was when all mosaic types were grouped together. When they looked at results for low/high level mosaic, there were only differences for the high level mosaic group:
- Euploid embryos (represented 84.7% of embryos transferred):
Ongoing pregnancy/live birth rate 60.2% - Low-level mosaic embryos (<50% abnormal cells, represented 10.6% of embryos transferred):
Ongoing pregnancy/live birth rate 55.6% (no statistical difference vs euploid, p= 0.0503). - High-level mosaic embryos (>50% abnormal cells, represented 3.8% of embryos transferred):
Ongoing pregnancy/live birth rate 46.5% (lower vs euploid, p< 0.001).
Based on this, high-level mosaics largely drove the overall difference seen between euploid and mosaic groups. Low-level mosaic embryos had live birth rates much closer to euploid embryos.
Mosaic status was a weaker predictor than standard embryo and patient features
To determine whether mosaic results meaningfully improve embryo selection, the researchers performed multivariable analyses that included standard predictors of IVF success like embryo grading and day of biopsy.
After adjustment, mosaic status was associated with live birth, but with a weaker effect compared to other factors. You can see the different factors below that were included in the multivariable analysis, ordered by how strongly each was associated with live birth.
- Day of biopsy (strongest factor associated with live birth)
- Number of prior embryo transfer failures
- Embryo morphology score
- Female BMI
- Mosaic status present
- Female age (weakest factor — this might seem unusual but remember, they’re mainly transferring euploids here, so the impact of age is low).
This shows that mosaic status was more weakly associated with live birth compared to traditional embryo and patient features.
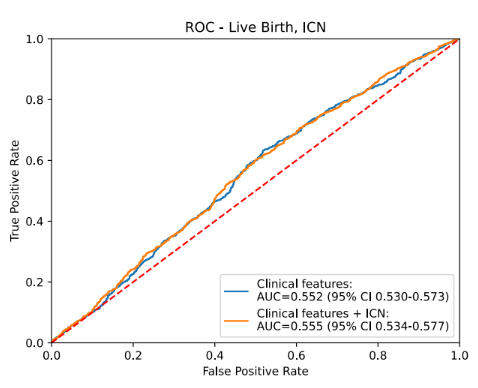
Next, the researchers tested whether adding mosaic results improved the ability to predict live birth. Using ROC curve analysis, they compared models based on standard embryo features (such as embryo quality and day of biopsy) with models that also included mosaic status. The curves were nearly identical, showing that mosaic results did not meaningfully improve live birth prediction beyond standard embryo selection factors.
The above results were based on the primary US group. All of these experiments were repeated in a separate European group, which used the same study design and showed similar results and conclusions.
Obstetric and neonatal outcomes were similar after euploid and mosaic transfers
The study also examined obstetric and neonatal outcomes among pregnancies.
Across both the US and European cohorts, no meaningful differences were observed between euploid and mosaic embryo transfers for:
- Gestational hypertensive disorders
- Gestational diabetes
- Placental complications
- Preterm delivery
- Low birth weight
- NICU admission
- Congenital anomalies
This suggests that mosaics did not increase the risk of adverse obstetric or neonatal outcomes compared with euploid embryo transfers.
Conclusion
In this study, embryos were transferred without clinics knowing whether mosaic results were present. This helped reduce bias and allowed the researchers to see how embryos actually performed when selected using standard criteria like embryo grading and day of biopsy.
Overall, euploid embryos had slightly higher live birth rates than embryos with mosaic results. However, this difference was mainly driven by a small group of embryos with high-level mosaic results. Low-level mosaic embryos had live birth rates much closer to euploid embryos.
In a statistical analysis, they also found that mosaic status was a weaker predictor of success than routine factors like embryo quality, day of biopsy, and prior failed transfers. When mosaic results were added to prediction models, they did not improve the ability to predict live birth.
The same findings were seen in a separate European group, which supports the reliability of the results.
Taken together, this study suggests that while some mosaic findings are linked to lower success rates, routinely reporting mosaic results doesn’t meaningfully improve embryo selection or clinical decision-making, beyond standard criteria like embryo grading and day of biopsy.
The authors note that, based on their study and other studies, routine mosaic reporting may do more harm than good. Mosaic results can cause unnecessary stress for patients and lead to viable embryos being discarded or deprioritized, while differences in how labs define mosaicism have added confusion, leading to skepticism about the value of PGT-A. “This skepticism could be reduced by discontinuing mosaicism reporting and adopting an evidence-based approach that focuses solely on uniform aneuploidy,” the authors write.
Note that this was a real-world study that included all embryos available for transfer, most of which were euploid (about 90%), with mosaic results being relatively uncommon. Because high-level mosaic embryos made up only a small fraction of transfers, their lower success rates had little impact on overall outcomes or prediction models, which explains why mosaic status didn’t improve multivariable or ROC analyses. If mosaic embryos were more evenly represented, the differences might appear larger, but that wasn’t the question this study set out to answer. Instead, the study asked whether mosaic reporting meaningfully improves embryo selection at the clinic level, across all patients and embryos, and found that it doesn’t. This doesn’t mean high-level mosaic findings have no effect, but rather that they are uncommon and their impact is modest, reinforcing that PGT-A’s main clinical value lies in identifying clearly aneuploid embryos rather than in routine reporting mosaic results.
Want to read more about PGT-A and mosaic embryos?

This post covers mosaic embryos, including their definition, frequency after PGT-A, mosaic embryo levels (low level, high level), mosaic embryo types (whole chromosome, segmental), current guidelines for transfer, potential for self-correction, and success rates. Read more.
Using a new non-toxic imaging method, researchers watched living human embryos divide in real time and discovered that chromosome separation errors linked to mosaicism can arise even at the blastocyst stage, showing that mosaicism is a dynamic process rather than one confined to early development. Read more.
A 2025 opinion article highlights some of the issues with PGT-A, mainly its uncertain benefit, technical flaws, high costs, and the risk of discarding potentially viable embryos. Read more.
A 2025 study re-analyzed embryos that tested as mosaic by NGS-based PGT-A using SNP karyotyping and found that one-third of those "mosaics" were actually uniformly aneuploid. Read more.
Reference
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Related posts:
 Complete guide to PGT-A (PGS testing)
Complete guide to PGT-A (PGS testing)
 Complete guide to mosaic embryos
Complete guide to mosaic embryos
 Ranking 1,000 mosaic embryo transfers
Ranking 1,000 mosaic embryo transfers
 No difference in euploid and mosaic embryo transfers: a clinical trial
No difference in euploid and mosaic embryo transfers: a clinical trial
 A look at how PGT-A results change with age, using data from over 86,000 biopsies
A look at how PGT-A results change with age, using data from over 86,000 biopsies
 Depletion of aneuploid cells in mosaic embryos
Depletion of aneuploid cells in mosaic embryos
 PGDIS releases 2021 guidelines for mosaic embryo transfers
PGDIS releases 2021 guidelines for mosaic embryo transfers
 ASRM’s 2024 committee opinion on the use of PGT-A
ASRM’s 2024 committee opinion on the use of PGT-A