A 2025 opinion article highlights some of the issues with PGT-A, mainly its uncertain benefit, technical flaws, high costs, and the risk of discarding potentially viable embryos.
In a recent 2025 article, Stéphane Viville and Mohamed Aboulghar take a hard look at PGT-A and ask whether it’s really helping couples undergoing IVF. They raise a number of points and I’ll share some of them here, which I’ll comment and elaborate on based on my knowledge/experience as a former embryologist and creator of this website.
For more background reading, check my Complete guide to PGT-A.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
PGT-A studies tend to focus on good prognosis patients, often not showing a clear benefit
Generally, randomized controlled trials that investigate PGT are done in good prognosis patients and on the basis of embryo transfer results. Viville and Aboulghar argue that the embryo transfer metric doesn’t consider the patients that don’t have embryos for transfer, including poor responders who don’t make many eggs. Looking at a “per retrieval” metric can be more revealing, as it includes the patients who couldn’t do PGT because they didn’t produce blastocysts. Viville and Aboulghar note that this is particularly important considering PGT is often recommended for older patients, who tend to produce fewer eggs compared to younger patients.
The authors referenced a 2020 Cochrane review that combined 13 RCTs up to 2019. I don’t think this Cochrane review is particularly useful, because many of the included studies use FISH — an outdated PGT technique that only assesses a few chromosomes. The authors of this review found that FISH for PGT is “probably harmful,” as it lowered live birth rates.
Since 2019, there have been two more RCTs:
- Munne et al. (2019) used NGS for PGT-A (the current standard) and found no difference in ongoing pregnancy rates or miscarriage rates between patients who transferred a euploid or their best quality embryo. Women 25-40 were included, with an average age of 33.7, and had good quality blastocysts. A post hoc analysis found that women aged 35-40 had an increased ongoing pregnancy rate with a euploid transfer (51% vs 37%). I reviewed this study in my post PGT-A doesn’t improve success rates in good prognosis patients.
- Yan et al. (2021) used NGS for PGT-A and found no difference in cumulative live birth after up to three embryo/euploid transfers within 1 year (77.2% vs 81.8%). They found lower miscarriage rates with PGT-A (8.7% vs 12.6%). The women were between 20-37 years old, and had at least 3 good quality blastocysts. I reviewed this study in my post PGT-A vs embryo grading: results of a 2021 clinical trial.
Based on the above data and a few other RCTs, the ASRM states that better RCTs are needed that investigate a broader range of patients, to see if there are benefits for the general population. You can read more about this in my post ASRM’s 2024 committee opinion on the use of PGT-A.
I’ll note that these studies are all looking at how a PGT-A tested euploid compares against a patient’s best quality untested embryo, with these recent RCTs finding no difference. The true value of PGT-A may be in identifying aneuploid embryos and avoiding the transfer of these embryos. Viville and Aboulghar don’t discuss this, which I think is a strong argument for the use of PGT-A. However, as we’ll see below, even aneuploid embryos can lead to successful pregnancies, albeit at a low rate.
PGT-A can lead to the discarding of potentially viable embryos
Mosaic embryos work!
Viville and Aboulghar describe how mosaic embryos came on the scene in 2015, as next-generation sequencing (NGS) started becoming more routinely used (aka PGT 3.0 — check here if you’d like to learn more about the history of PGT-A). This was when I started work as an embryologist, so I have first-hand experience with this period in PGT’s history! I also started this website around then (2018).
Mosaic embryos have a mix of euploid and aneuploid cells:
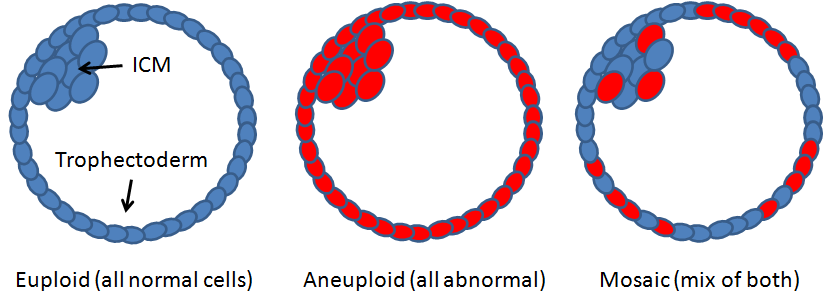
There was a lot of uncertainty with mosaics, leading most labs to discourage their transfer until more was known. Different guidelines were put together, namely those put out by the PGDIS in 2019 that prioritized mosaics based on the specific chromosome(s) affected. This led to many mosaics being discarded, as most labs refused to transfer a mosaic that could potentially lead to a baby with a syndrome (ie. a trisomy 21 mosaic might lead to Down syndrome). It’s worth pointing out that couples who never do PGT often transfer these mosaics unknowingly, which was one way for doctors to rationalize transferring these embryos in the absence of data.
It took a few years for research to come out that showed that these mosaics could lead to a live birth without the same chromosomal abnormality. An important study by Viotti et. al (2021) (reviewed here) transferred 1000 mosaics, finding that the % mosaicism was linked to mosaic success rates, with low level mosaics performing better than high level mosaics (and low/moderate level mosaics being comparable to euploids, as reviewed here). This changed PGT-A from providing a simple euploid/aneuploid diagnosis to something more like a gradient.
This research led to a change in guidelines, with ESHRE, the ASRM and PGDIS prioritizing mosaic transfers based on % mosaicism rather than the specific chromosome. You can read more about that in my post Guidelines for prioritizing mosaics for embryo transfer.
Even as these guidelines have evolved to allow mosaic embryo transfers, some clinics are still reluctant to transfer them. This leads to embryos with real potential being discarded to this day!
To learn more about mosaics and their success rates, check my Complete guide to mosaic embryos.
Aneuploid embryos work too, but rarely
The whole point of PGT-A is to identify euploid, mosaic and aneuploid embryos to prioritize transfer. On the bottom of this ranking order are aneuploid embryos, which are believed to have a high chance of failing to implant or miscarry. These embryos aren’t recommended for transfer and are usually discarded.
So do they work?
I’ve summarized the most up-to-date data across multiple studies here: Aneuploid embryo success rates after transfer, which suggests live birth rates are very low (~1%) but not zero. Here’s a closer look at a couple of the studies:
- A 2020 study (reviewed here) transferred 414 embryos that were biopsied but not tested until after the pregnancy result was known. There were 102 aneuploid transfers, with 24 resulting in a pregnancy, but none of them led to a live birth.
- A 2025 case report (reviewed here) describes the healthy birth of dizygotic twin girls from embryos labeled as aneuploid by PGT-A.
This suggests that aneuploid embryos rarely work and are at a high risk of miscarriage. However, there aren’t many studies looking at this, so more work is needed!
The reason these embryos work might be because they’re actually mosaic, and that a single biopsy isn’t representative of the whole embryo (discussed more in the next section).
Because of the discarding of mosaic and aneuploid embryos, Viville and Aboulghar argue that PGT-A can only decrease the cumulative live birth rate.
A single biopsy isn’t representative of the whole embryo
When a biopsy for PGT is performed, around 5-10 cells from the trophectoderm are taken. This biopsy is meant to represent the whole blastocyst, which could be hundreds of cells in size.
Studies have shown that rebiopsying an embryo often leads to different results (non-concordance). As reviewed in my post Does a PGT-A biopsy match the rest of the embryo?, about 80% of aneuploids give the same result after a second biopsy, 94% for euploids and only 43% for mosaics. This suggests that a single biopsy may not enough to represent the embryo. Below you can see an illustration of this and how a second biopsy can give different results.

Furthermore, these results are from trophectoderm rebiopsies. The ICM, which is the part of the blastocyst that becomes the fetus, is never biopsied for PGT-A because this would kill the embryo. It’s possible that the ICM can have a different result than the trophectoderm.
There’s been other studies that have gone a step further and sequence the DNA of all the cells in an embryo — ICM and trophectoderm!
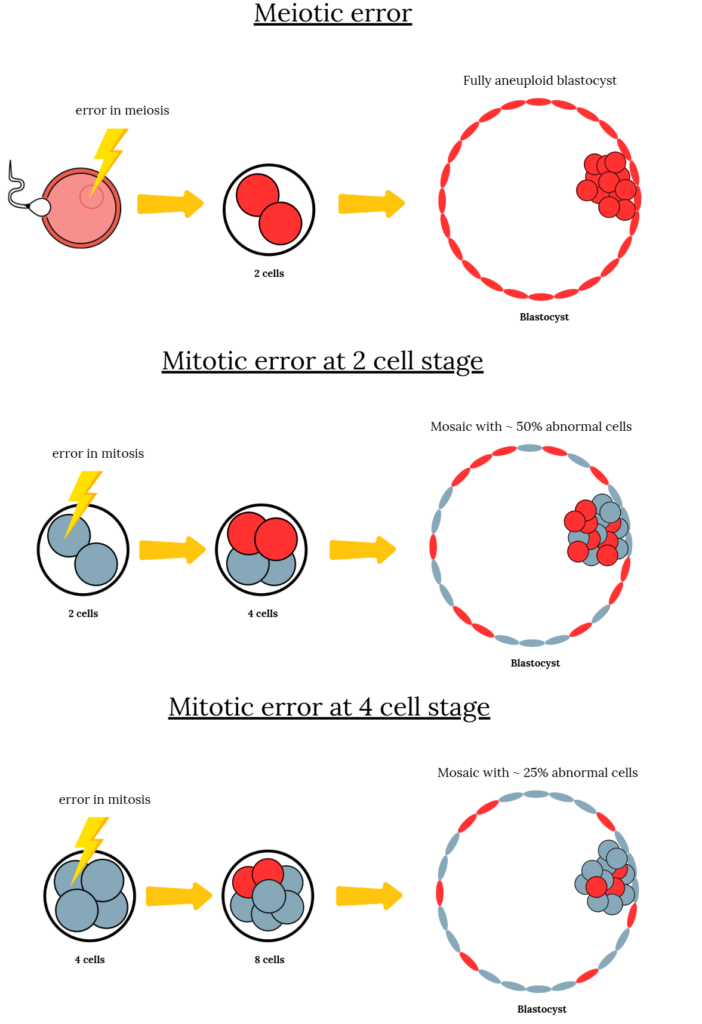
Using this technique, one study (reviewed here) showed that 82% of tested embryos were mosaic, while another (reviewed here) found that nearly all blastocysts and fetal tissue samples were mosaic! Recently, a mathematical model predicted that fully euploid embryos are rare, while aneuploid or mosaic embryos are much more common (reviewed here). This is because errors in the sperm or egg (errors of meiosis) are carried over to the embryo, making all cells aneuploid, while a euploid embryo inevitably has a hard time remaining a euploid as its cells could accumulate errors as it divides (errors of mitosis).
PGT-A is expensive
Viville and Aboulghar, in their article, bring up a good point that I rarely see discussed in PGT-A research: the high price! According to Goldman et al. 2018, patients typically spend about $30,000 for a 90% chance of obtaining a euploid.
Researchers in a 2024 study (reviewed here) compared the costs of patients with or without PGT-A, finding that patients younger than 35 may not benefit because of the higher chance of top-graded embryos being euploid anyway.
Viville and Aboulghar argue that these high costs not only place a significant financial burden on couples but can also compromise patient autonomy, pushing couples to using PGT-A potentially against their best financial and medical interests. This financial burden might also limit the number of IVF cycles a couple is able to afford, potentially reducing their overall chance of success.
Euploid embryos don’t always work
Many patients believe having a euploid embryo is a guarantee, but this isn’t true!
Here’s a list of reasons euploid embryos might not work:
- Besides the embryo, the uterine environment is also important for implantation. Some patients might have endometritis or endometriosis that could disrupt implantation.
- PGT-A can’t detect small changes in DNA. Some embryos might have genetic mutations that affect their normal development that are too tiny to be detected by PGT-A.
- A 5-10 cell biopsy might not be representative of the whole embryo, which could be hundreds of cells. It’s possible that the “euploid” transferred is actually a mosaic that didn’t self-correct.
- Embryo quality, and the day the embryo was biopsied, still matter. Good quality euploids have a better chance than poor quality euploids; day 5 euploids have a better chance than day 7.
- The proficiency of the embryology team and the doctor that performs the transfer also matters.
A 2023 study combined the results of 74 studies to investigate what factors contribute to euploid live birth and miscarriage rates, identifying embryo quality, maternal age, specific diagnoses, repeat freeze/thaw, and other factors. You can read more in my post Meta-analysis combines 74 studies to examine factors linked to euploid transfer success.
Conclusions
In the end, Viville and Aboulghar write that despite its promise, PGT-A has not lived up to expectations. Its uncertain benefits, combined with technical flaws, high costs, and the risk of discarding potentially viable embryos, suggest that the test might not be as helpful as once believed.
For reasons like this, major organizations like the HFEA, ESHRE and the ASRM do not recommend the routine use of PGT-A.
“Ultimately, we suggest that PGT-A should no longer be offered to infertile couples,” Viville and Aboulghar conclude.
However, this is a debated position, and in my opinion, the value of the test is in its ability to identify aneuploid embryos so these embryos aren’t prioritized for transfer. Current evidence suggests that these embryos have low potential, although there aren’t many studies on this topic and more research is needed. This may be particularly relevant for older patients who have a lot of embryos, as research has shown that the chance of producing an aneuploid embryo increases with age (reviewed here). However, high quality studies that assess the benefit of PGT-A in this patient group are lacking.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Trophectoderm and ICM biopsies match depending on the abnormality
Trophectoderm and ICM biopsies match depending on the abnormality
 Does a PGT-A biopsy match the rest of the embryo?
Does a PGT-A biopsy match the rest of the embryo?
 Mosaicism much more common than previously thought, using more sensitive PGT-A technique
Mosaicism much more common than previously thought, using more sensitive PGT-A technique
 More sensitive PGT-A test shows that nearly all blastocysts, fetal tissues are mosaic
More sensitive PGT-A test shows that nearly all blastocysts, fetal tissues are mosaic
 Mathematical model predicts that fully euploid embryos are rare
Mathematical model predicts that fully euploid embryos are rare
 Real-time imaging suggests that embryo mosaicism may change over time
Real-time imaging suggests that embryo mosaicism may change over time
 ASRM’s 2024 committee opinion on the use of PGT-A
ASRM’s 2024 committee opinion on the use of PGT-A
 Chromosomal errors in IVF: What is aneuploidy and what causes it?
Chromosomal errors in IVF: What is aneuploidy and what causes it?