
Researchers in a 2023 study combined the results of 74 studies to investigate what factors contribute to euploid live birth and miscarriage rates, identifying embryo quality, maternal age, specific diagnoses, repeat freeze/thaw, and other factors.
Euploid embryo transfers tend to have higher success rates, however different factors contribute to whether or not they implant and lead to a live birth.
Cimadomo et al. (2023) performed a systematic review and meta-analysis and combined the results of 74 studies to better understand the factors associated with live birth and miscarriage rates when transferring a euploid embryo. They examined embryonic, maternal, paternal, clinical and lab factors.
For more background information on PGT-A, check out my Complete guide to PGT-A (PGS testing).
To better understand this article, be sure to check out the glossary entries for “odds ratio” and “heterogeneity.”
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- Prospective and retrospective studies were included, as well as randomized controlled trials.
- Only euploids were included, no mosaic embryos.
- Different PGT-A technologies were used depending on the study (aCGH, qPCR, SNP, NGS).
- Miscarriage rate was defined as a spontaneous loss before 22 weeks.
- Most studies involved single euploid transfers, but some involved double transfers.
Embryonic factors that contribute to live birth in PGT-A
A number of embryonic factors were looked at in this study, with the results of the meta-analysis indicated below. Euploids with a C grade ICM or trophectoderm had lower live birth rates than an embryo with an A or B grade, and euploids graded as poor quality (<BB) had lower birth rates than those of higher quality. Additionally, embryos that were biopsied on day 5 had higher live birth rates compared to those biopsied on day 6 or 7.

In terms of miscarriage rates, studies with a grade C trophectoderm showed an increase (17.0% vs 13.3%, odds ratio [95% CI]: 1.44 [1.09-1.90]; 7 studies, I2= 10%), and studies comparing day 5 and day 6/7 embryos had an increase (16.9% vs 12.4%, odds ratio [95% CI]: 1.49 [1.25-1.76]; 13 studies, I2= 0%).
Additional selected information that wasn’t included in the meta-analysis:
- Bradley et al. (2017) found that euploids derived from 2PN or 1PN fertilized eggs showed no difference in live birth rates.
- Balakier et al. (2016) found that euploids from multinucleated embryos on day 2 showed a lower birth rate.
- Pons et al. (2019) found that euploids from day 3 embryos with <8 cells had lower live birth rates.
- Lagalla et al. (2020) found that euploids from partially compacted morulas had no differences in live birth rates.
- A total of 13 studies were examined that dealt with mitochondrial DNA levels in euploids. The authors noted a large amount of heterogeneity and a lack of normalization in the results, which prevented them from including the studies in the meta-analysis.
Maternal factors that contribute to live birth in PGT-A
You can see the results of maternal factors and live birth rate after euploid transfer below. Women 38 or older had a lower live birth rate, as did those diagnosed with recurrent implantation failure (RIF) those with a BMI 30 and above. There were no differences in the other diagnoses (unexplained infertility, polycystic ovarian syndrome, diminished ovarian reserve, endometriosis, tubal factor, recurrent pregnancy loss) or in those using the endometrial receptivity array (ERA).
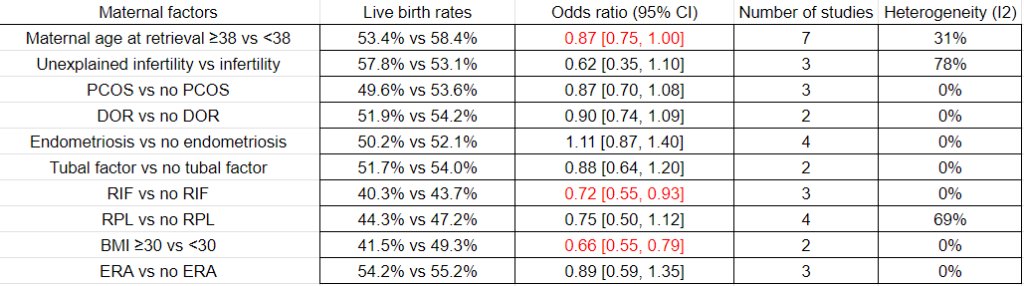
In terms of miscarriage rates, there was only an increase in women with a BMI 30 and above vs those with a lower BMI (18.7% vs 11.0%, odds ratio [95% CI]: 1.80 [1.08-2.99]; 2 studies, I2= 52%).
Additional selected information that wasn’t included in the meta-analysis:
- Neal et al. (2020) found similar live birth rates in women with and without adenomyosis.
- For estradiol levels, one study looked at max E2 levels during ovarian stimulation and found no difference in live birth rate (Irani et al. 2020).
- Green et al. (2015) compared euploid transfer outcomes in women with different thyroid stimulating hormone levels (ranging from <0.5 to >2.5 mIU/L) and found no differences in live birth rates. There was also no difference in women who did or didn’t take levothyroxine.
Paternal factors that contribute to live birth in PGT-A
You can see the results of paternal factors and live birth rate after euploid transfer below. There were no differences in live birth rates in terms of paternal age or male factor.

There were no differences in miscarriage rates with these paternal factors.
Additional selected information that wasn’t included in the meta-analysis:
- Several studies on sperm DNA fragmentation have been done but couldn’t be included in the meta-analysis because they reported ongoing pregnancy rates (and not live birth rates). None of the studies found a difference in euploid transfers.
Clinical and lab factors that contribute to live birth in PGT-A
You can see the results of clinical/lab factors and live birth rate after euploid transfer below. Embryos that were hatched for biopsy at the same time as the biopsy had a higher live birth rate compared to those hatched on day 3, and embryos that were biopsied once/frozen twice had a lower live birth rate compared to biopsied once/frozen once embryos. There were no differences in gonadotropin dose, type of ovarian stimulation trigger, fresh vs frozen eggs, embryos rebiopsied, and medicated vs modified natural frozen embryo transfers (FETs).
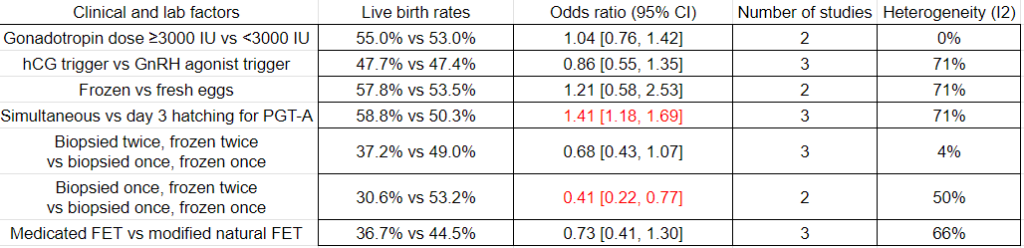
There were no differences in miscarriage rates with these clinical/lab factors.
Additional selected information that wasn’t included in the meta-analysis:
- De Munck et al. (2020) found similar euploidy rates for IVF vs ICSI.
- Munne et al (2017) found that different IVF clinics had different euploidy rates in donor eggs.
- Guzman et al. (2018) reported that larger biopsy sizes resulted in reduced implantation rates.
- Several studies examined live birth rates of euploid transfers among different IVF centers and found no differences.
Conclusions
This study found that euploid transfers resulted in decreased live birth rates with:
- Grade C ICM
- Grade C trophectoderm
- Poor quality embryos
- Day 6/7 embryos
- Maternal age ≥38
- Recurrent implantation failure
- BMI ≥30
- Hatching embryos on day 3 (vs simultaneous hatching and biopsy)
- Embryo refreezing
While miscarriage rates increased with:
- Grade C trophectoderm
- Day 6/7 embryos
- BMI ≥30
They didn’t find differences in live birth rate due to:
- Unexplained infertility
- PCOS
- DOR
- Endometriosis
- Tubal factor
- Recurrent pregnancy loss
- ERA
- Paternal age
- Male factor
- Gonadotropin dose
- Type of ovarian stimulation trigger
- Rebiopsied embryos
Since most of the data was retrospective, the quality of evidence was low to very low. This is a limitation of the meta-analysis, and most of the data should be verified using randomized controlled trials.
Due to the limited number of studies, another limitation is that different PGT-A technologies were combined. However, the researchers were adamant in not using studies that involved mosaic embryos, opting only for euploid results, which may be more consistent across PGT-A technologies.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 An Italian consensus on key performance indicators for assessing IVF clinics
An Italian consensus on key performance indicators for assessing IVF clinics
 ASRM’s 2024 committee opinion on the use of PGT-A
ASRM’s 2024 committee opinion on the use of PGT-A
 Complete Guide to Embryo Grading and Success Rates
Complete Guide to Embryo Grading and Success Rates
 Predicting live birth rates, multiples based on 223,377 transfers
Predicting live birth rates, multiples based on 223,377 transfers
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?
 Study evaluates factors affecting pregnancy outcomes after euploid transfer
Study evaluates factors affecting pregnancy outcomes after euploid transfer
 Study compares PGT-A outcomes for patients with different diagnoses
Study compares PGT-A outcomes for patients with different diagnoses
 Study estimates number of frozen eggs needed for euploids, live births
Study estimates number of frozen eggs needed for euploids, live births